A rejuvenation therapy and sulforaphane focused on the study’s clinical biomarkers and not its biological age measurements. This Part 2 curation of the study highlights its epigenetic clocks because:
“While clinical biomarkers have obvious advantages (being indicative of organ dysfunction or disease), they are neither sufficiently mechanistic nor proximal to fundamental mechanisms of aging to serve as indicators of them. It has long been recognized that epigenetic changes are one of several primary hallmarks of aging.
DNA methylation (DNAm) epigenetic clocks capture aspects of biological age. The discrepancy between DNAm age and chronological age (term as ‘epigenetic age acceleration’) is predictive of all-cause mortality. Pathologies and conditions that are associated with epigenetic age acceleration includes, but are not limited to, cognitive and physical functioning, centenarian status, Down syndrome, HIV infection, obesity, and early menopause.
The [new] human-rat clocks apply to both species. The two human-rat pan-tissue clocks are distinct, by way of measurement parameters. One estimates absolute age (in units of years), while the other estimates relative age, which is the ratio of chronological age to maximum lifespan; with values between 0 and 1. This ratio allows alignment and biologically meaningful comparison between species with very different lifespan (rat and human), which is not afforded by mere measurement of absolute age.
Relative age estimation was made using the formula: Relative age = Age / maxLifespan where the maximum lifespan for rats and humans were set to 3.8 years and 122.5 years, respectively.”
From Supplementary Table 3, old control and old treatment subjects were males 109 weeks old, 55% of their maximum lifespan (109 / 197.6). Young control subjects were males 30 weeks old, 15% of their maximum lifespan.
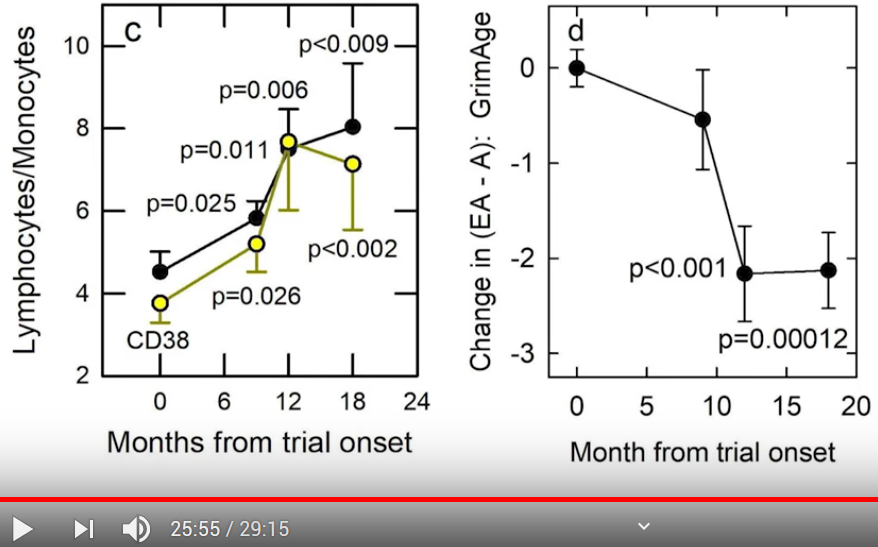
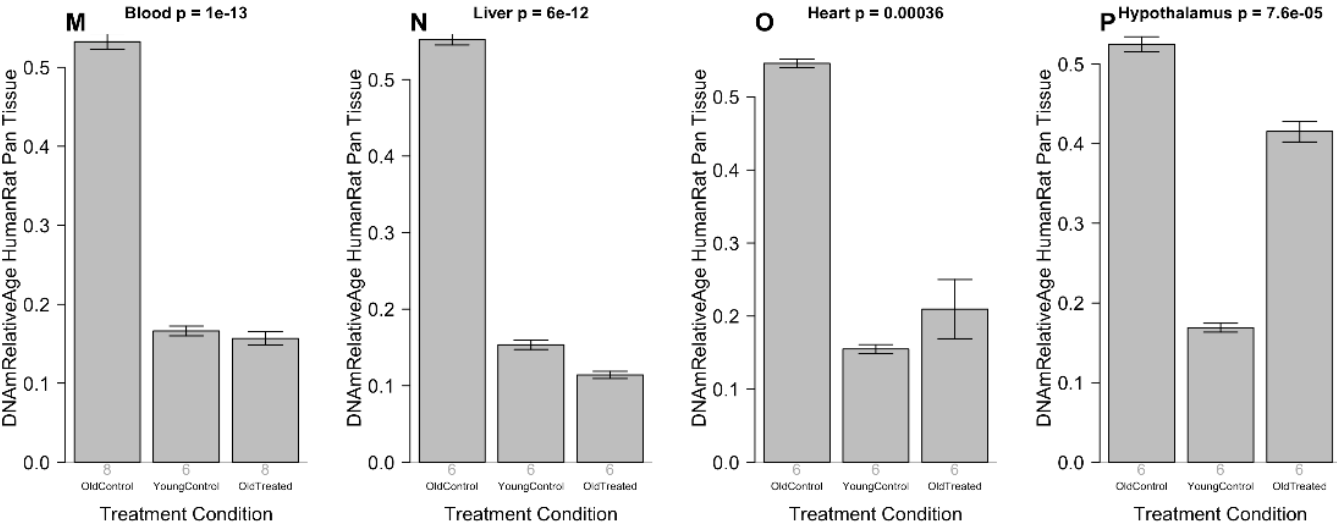
The money charts for this study’s human aging applications – measured by the new human-rat relative biological age clock – were buried in Supplementary Figure 12, bar plots M through P:
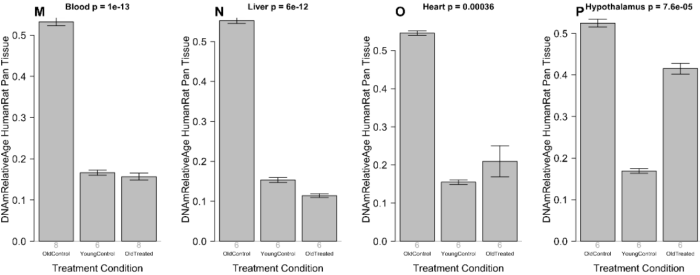
“Human-rat clock measure of relative age defined as age/maximum species lifespan. Each bar-plot reports the mean value and one standard error.”
From Supplementary Table 8, the percentages of rejuvenation for the above bar plots, calculated as “(100 * (1 – Old Treated / Old Control)” were:
- “Blood 70.6%
- Liver 79.4%
- Heart 61.6%
- Hypothalamus 20.9%”
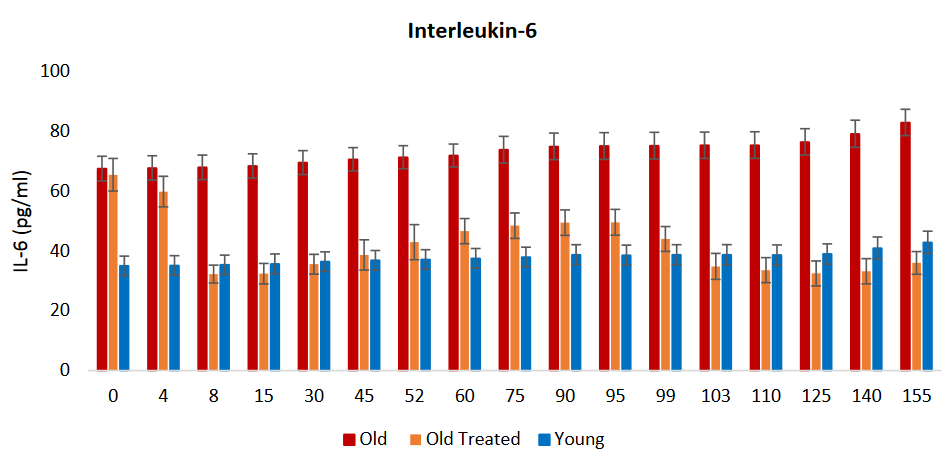
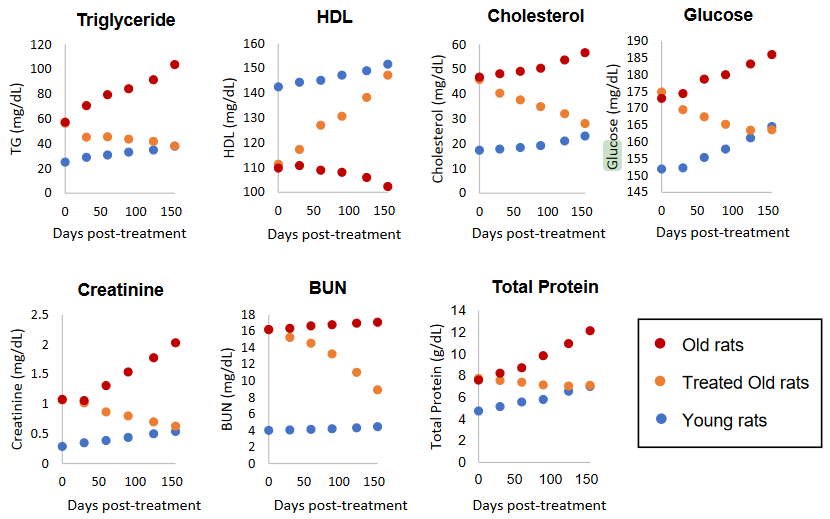
Let’s return to clinical biomarkers for comparison purposes. The current study measured pro-inflammatory cytokine IL-6 blood plasma levels at every time point, but didn’t publish numbers. Bar plots and narrative were:
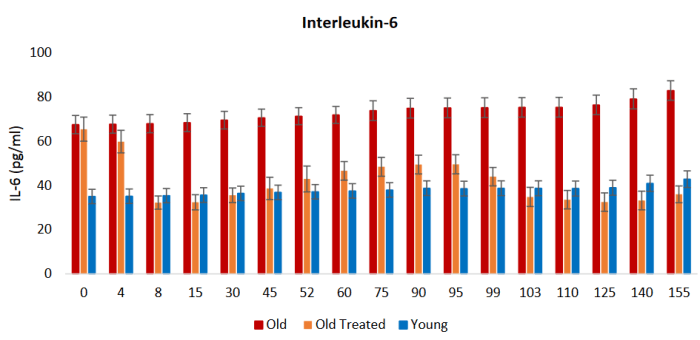
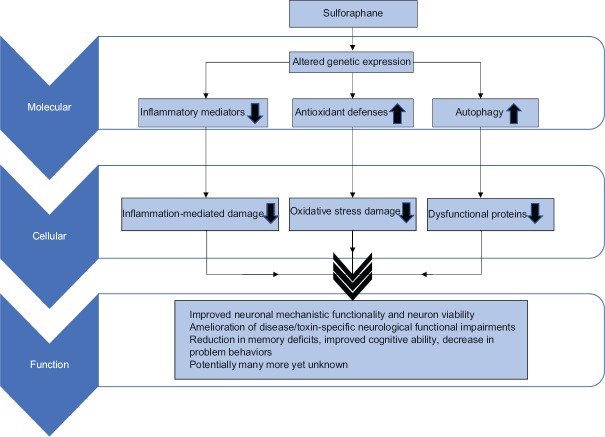
“Inflammation is an important response that helps protect the body, but excess inflammation especially in terms of duration of this response can have very detrimental effects instead. This occurs when inflammation fails to subside and persists indefinitely; a condition referred to as chronic inflammation, which for reasons not well-understood, increases with age and is associated with a multitude of conditions and pathologies.
The levels of two of the most reliable and common biomarkers of chronic inflammation, interleukin 6 (IL-6) and tumor necrosis factor α (TNF-α), are found to be considerably higher in old rats, and these were very rapidly diminished, within days by plasma fraction treatment, to comparable levels with those of young rats. This was especially stark with IL-6.
In time, the levels of these inflammatory factors began to rise gradually, but they were once again very effectively reduced following the second administration of the plasma fraction on the 95th day.”
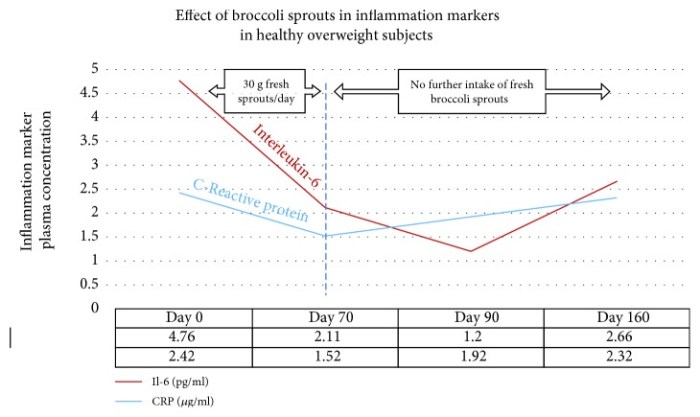
Let’s compare the above IL-6 graphic with IL-6 concentration improvements of our 2018 model clinical trial, Effects of long-term consumption of broccoli sprouts on inflammatory markers in overweight subjects, calculated as (100 * (1 – Day _ mean / Day 0 mean):
Mean pg/ml | % improvement | Period | Broccoli sprout consumption
- 4.594 | 0% | Day 0 | “One week before the beginning of the intervention period, subjects were asked to avoid the consumption of Brassica vegetables (broccoli, radish, cauliflower, Brussel sprouts, mustards, among others) and their derived products.”
- 1.748 | 62.0% | Day 0 to 70 | Subjects ate 30 g raw broccoli sprouts every day, and stopped eating them after Day 70.
- 0.896 | 80.5% | Day 0 to 90 | “After the intervention period, a follow-up recovery period for all subjects continued for another 90 days with no ingestion of broccoli sprouts.”
- 2.170 | 52.8% | Day 0 to 160 | Subjects had not eaten broccoli sprouts after Day 70.
Results between the studies were similar in that:
- IL-6 levels improved during early treatments through rat Day 8 and human Day 70, respectively.
- IL-6 levels continued decreasing shortly after treatments for 7 days (through rat Day 15) and 20 days (through human Day 90), respectively.
- IL-6 levels rose after rat Day 15 and human Day 90, respectively, but were still significantly below Day 0 values at rat Day 95 and human Day 160.
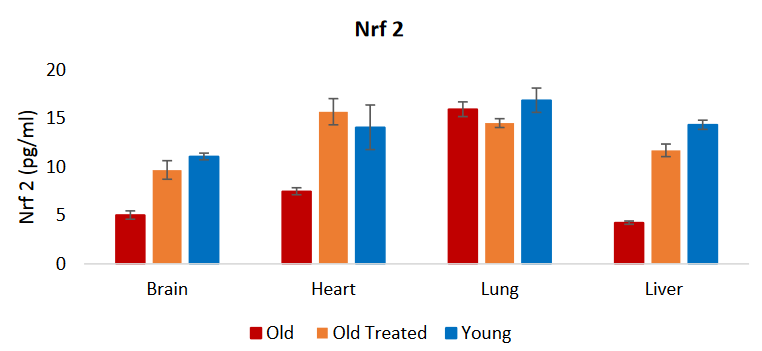
The current study measured Nrf2 but didn’t publish numbers. Bar plots and narrative were:
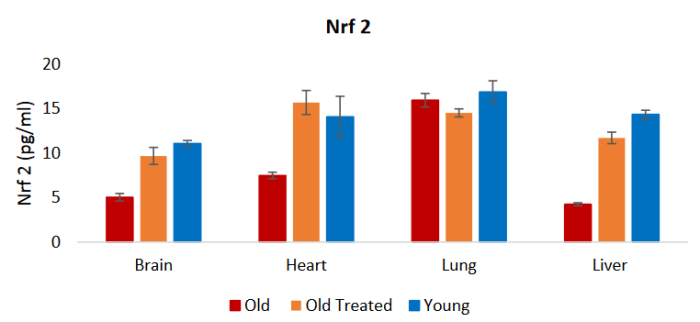
“The reduction of these inflammation markers is consistent with the profile of the nuclear factor erythroid 2-like 2 protein (Nrf2), which plays a major role in resolving inflammation, in part by inhibiting the expression of IL-6 and TNF-α. Nrf2 also induces the expression of antioxidants that neutralizes ROS [reactive oxygen species], which is also a significant feature in inflammation.”
A PubMed search on “nrf2 sulforaphane human” didn’t turn up relevant 2020 human in vivo studies. I disregarded reviews, cancer studies, disproven hypotheses, and other compounds listed in the below graphic.
I won’t repeat the entire Nrf2 section from the Part 1 curation, just one graphic and paragraph:

It [sulforaphane] is not only a potent Nrf2 inducer but also highly bioavailable [around 80%], so that modest practical doses can produce significant clinical responses. Other Nrf2 activators [shown in the above image] not only lack potency but also lack the bioavailability to be considered as significant intracellular Nrf2 activators.”
As noted in Reviewing clinical trials of broccoli sprouts and their compounds, there are no sulforaphane clinical trials that also use epigenetic clocks. Broccoli sprouts and their compounds’ effects on human aging is an area that hasn’t drawn attention and funding.
What effects may broccoli sprout compounds have on human aging? With this new human-rat relative biological age clock, researchers can get reliable answers from rat studies, with human clinical trials needed only to confirm those findings!
As rejuvenation research continues, what could people do easily, cheaply, and today for our long-term selves? Don’t know about the hypothalamus, but our blood, liver, and heart biological ages may decrease as we reduce inflammation and oxidative stress by eating broccoli sprouts.
I’m at a similar percentage of species maximum lifespan as were the study’s treated subjects. It’s my choice as to what my healthspan will be.
There isn’t evidence today to definitively say that changing my inflammatory phenotype with broccoli sprouts has had / will have rejuvenation effects on biological ages of my cells, organs, and body. But if eating broccoli sprouts every day not only reduces chronic inflammation and oxidative stress as expected, but also makes me younger, I could probably learn to live with that. 🙂
Continued with Part 3 of Rejuvenation therapy and sulforaphane.