A 2026 paper presented results of a clinical trial that selectively added myrosinase enzyme via mustard powder and vitamin C to measure in vivo effects on glucoraphanin conversion to sulforaphane:
“Effects of exogenous myrosinase (Myr) on conversion efficiency of glucoraphanin (GR) to sulforaphane (SF) was compared to gut microbial Myr-like activity. In a randomized, double-blind, crossover study, sixteen subjects (9 F: 7 M) received a single oral dose of GR in 385 mg broccoli seed extract (BSE) with 72.5 mg Myr-containing mustard seed powder, or broccoli seed extract alone, both with 100 mg ascorbic acid.
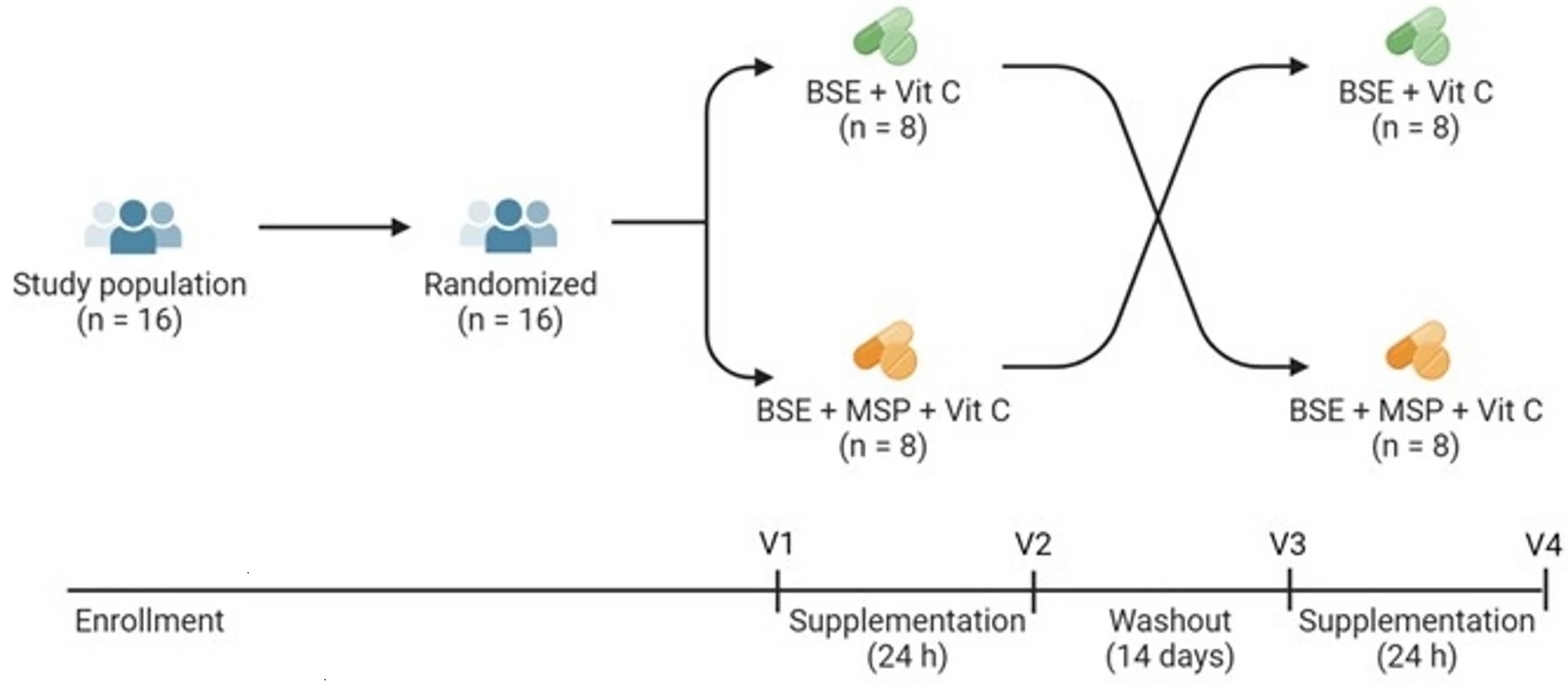
GR + Myr, on average, doubled the bioavailability of SF (39.8 ± 3.1%) compared to GR alone (18.6 ± 3.1%), and increased the conversion rate in the first 8 h (25.4% ± 2.7%) compared to GR alone (8.0% ± 2.7) based on measurement of urinary metabolites. The majority of subjects given GR as BSE with exogenous Myr and Vit C, converted GR to SF notably faster (e.g., within the first 8 h), than those given GR and Vit C alone.
One of the most likely explanations for the pronounced differences is that when SF was produced as a result of added exogenous Myr, it was produced and absorbed in the small intestine and metabolized primarily to its glutathione (GSH) derivatives and excreted in urine. This is a more rapid process than when GR passes into the large intestine and then is acted upon by the greater bacterial population within that terminal segment of the gastrointestinal system.
No differences were observed in the 8 to 24 h urine collection (Time 24 h) between the two treatments: 11.7 ± 1.3% for GR + Myr vs. 8.9 ± 1.3% for GR alone. Bacterial communities did not differ between low/high GR converters following supplementation.
Many bacteria which persist in the small intestine and upper large intestine, as well as in mucosal-associated fractions, are not well represented in feces. The lack of anatomically specific microbial communities in the human gut limits our knowledge of GR conversion in people.”
https://www.nature.com/articles/s41598-026-39389-4 “Exogenous myrosinase from mustard seed increases bioavailability of sulforaphane from a glucoraphanin-rich broccoli seed extract in a randomized clinical study”
1. Lost in this study’s shuffle was the reason why sulforaphane’s effects are beneficial in the first place. As Switch on your Nrf2 signaling pathway pointed out:
“We use N-acetylcysteine (NAC) in the lab all the time because it stops an Nrf2 activation. So that weak pro-oxidant signal that activates Nrf2, you switch it off by giving a dose of NAC. It’s a potent antioxidant in that right, but it’s blocking signalling. And that’s what I don’t like about its broad use.”
It’s relevant to the Nrf2 activating effects of sulforaphane when antioxidant vitamin C taken to increase myrosinase hydrolyzation of glucoraphanin to sulforaphane if this vitamin C dose may also block Nrf2 activation. An increase of sulforaphane and its metabolites wouldn’t physiologically matter if their beneficial effects were simultaneously blocked.
2. Another indicator that these researchers lost the plot was shown when they asserted: “These data suggest that the present study may not have included sufficient AA to optimize Myr enzyme activity in vivo, another consideration for future studies” based on comparing the in vitro Reference 21 ascorbic acid doses (0, 11, 44, 88, or 154 mg AA/capsule). I don’t have access to Reference 21 to see whether it also didn’t assess Nrf2 activation.
3. For comparison of this study’s 50 mg glucoraphanin dose on two non-consecutive days, the cited Our model clinical trial for Changing to a youthful phenotype with broccoli sprouts provided daily 30 grams of fresh broccoli sprouts that contained an estimated 51 mg of glucoraphanin for ten weeks. Although no broccoli sprout preparation or intake guidelines were enforced, unassisted glucoraphanin conversion to sulforaphane had many beneficial effects in that trial.
4. These researchers stated “No differences were observed in the 8 to 24 h urine collection (Time 24 h) between the two treatments.” Whether the faster small intestine absorption of sulforaphane had benefits over the slower large intestine absorption wasn’t investigated.
5. I’ve previously corresponded with one of this study’s coauthors, and think their research group could do better work without the retired broccoli sprout expert. Maybe they would take more confident ownership of their work if they let him ride off into the sunset, and decide for themselves what predictable findings would be in their research effort’s scope?
Maybe they wouldn’t let fester the same old issues in his papers? It doesn’t say anything good about current research if its main findings just repeat last decade’s findings.
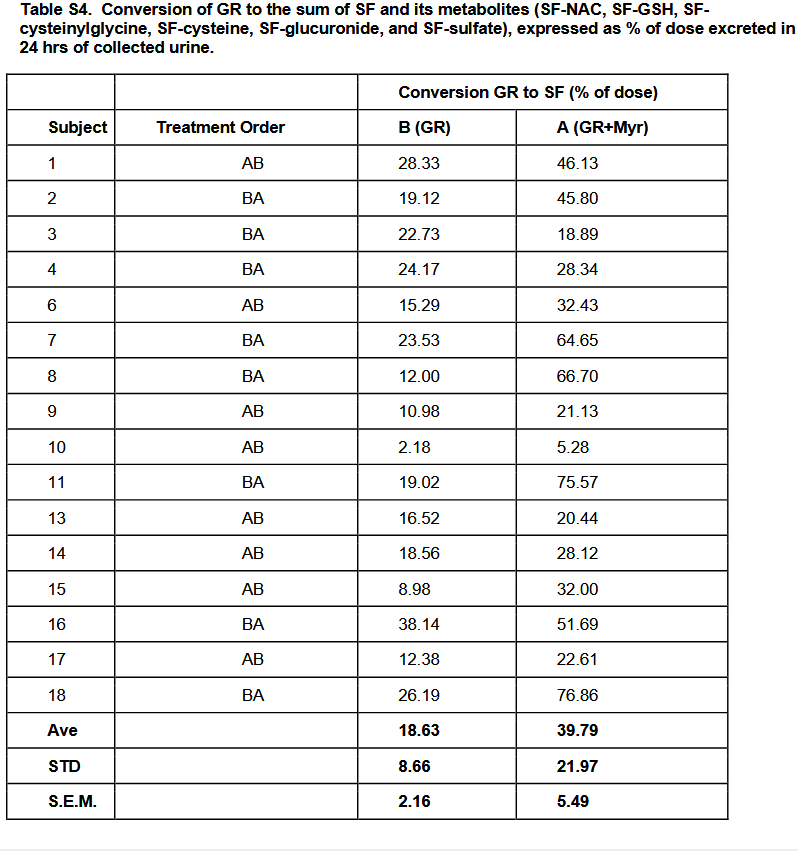
For example, Table S4 has stories that weren’t told. It conforms to the expert’s cited 2015 study findings, but presenting averages doesn’t reveal causes for individual differences. So questions on the individual level continue to be unanswered, such as:
- Subject 8 had more than a fivefold increase of glucoraphanin-only conversion to glucoraphanin + myrosinase conversion. What blocked the other subjects from achieving similar results?
- Why was Subject 10 so far behind everyone else’s capabilities? They would have had to increase their glucoraphanin-only conversion by fourfold just to get to the next lowest person’s level, Subject 15, but sixfold to get to Subject 15’s glucoraphanin + myrosinase conversion level.
6. Every researcher wants to have an impact on their field. The time to think over how to newly research possible impactful outcomes is before the study starts.
Since I’m in my seventh year of eating broccoli sprouts every day, I would have paid close attention to more rigorous bioavailability, more exact microbiota collection techniques, or detailed exploration of differences in people’s responses to the same treatments, all of which were predictable issues beforehand. I didn’t really care for listing them in the Discussion section, then dismissing investigations of these findings for some future research to explore.