People will forgive you for being wrong, but they will never forgive you for being right – especially if events prove you right while proving them wrong. Thomas Sowell
A 2026 primate study investigated effects of vitamin C:
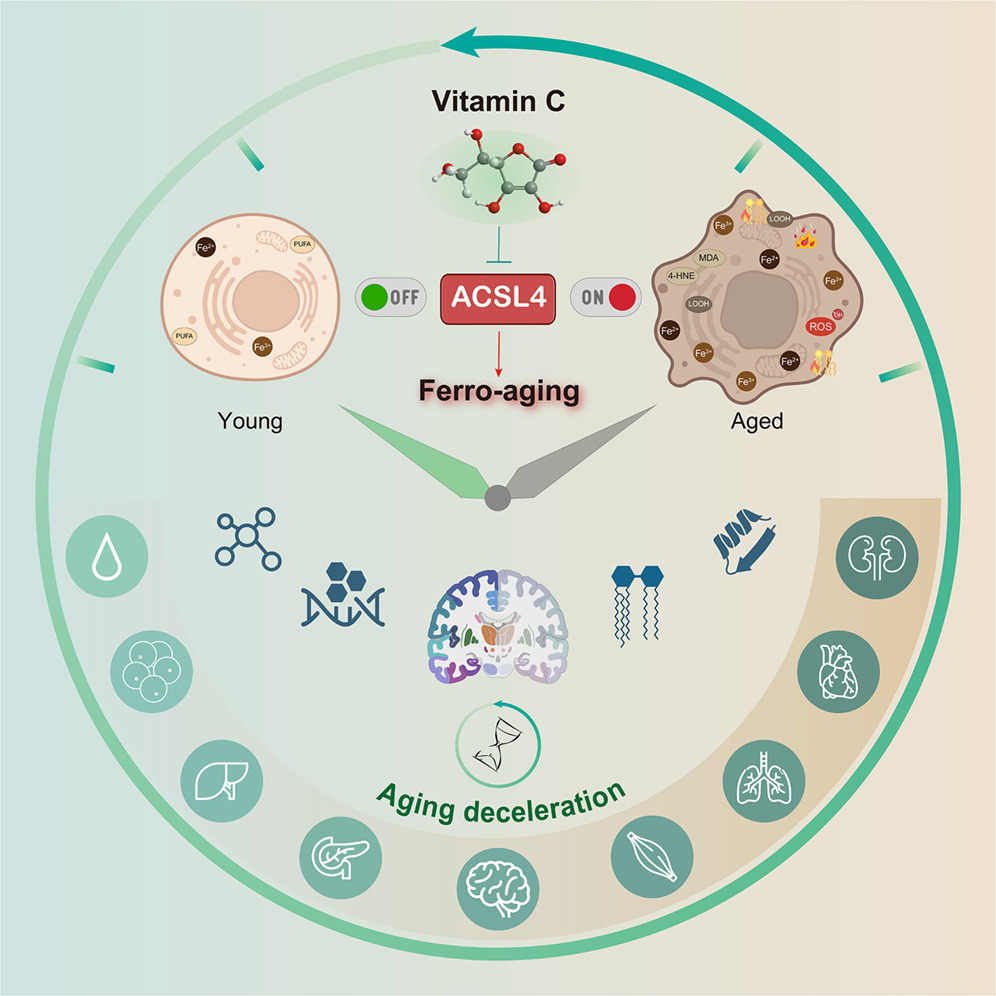
“Here, we define a conserved iron-lipid axis driving primate aging, termed ‘ferro-aging.’ Multi-tissue profiling in humans and non-human primates reveals age-progressive iron accumulation, fueling chronic lipid peroxidation orchestrated by acyl-coenzyme A (CoA) synthetase long-chain family member 4 (ACSL 4). Distinct from acute ferroptosis, this ACSL4-mediated process promotes cellular senescence and systemic functional decline.
We identify vitamin C (VC) as a direct inhibitor of ACSL4. Long-term VC administration in aged monkeys for over 40 months potently reduces ferro-aging signatures across tissues, attenuates multi-organ pathology, and improves neurological and metabolic functions. Multi-omic aging clocks indicate the VC-mediated reversal of biological age.
Despite decades of interest in oxidative stress, largely sparked by the free radical theory of aging, efforts to modulate it broadly with antioxidants have yielded inconsistent or neutral outcomes, highlighting the theory’s limitations and underscoring the need to identify more specific, upstream drivers. A critical challenge remains: determining whether the iron-lipid axis constitutes a core upstream driver of aging in primates and, if so, whether it is therapeutically targetable.
In this study, we bridge these gaps. We define an iron-triggered, ACSL4-governed, lipid peroxidation-driven program that escalates with age across diverse cell types and multiple organs in non-human primates.
VC treatment dose-dependently increased Nrf2 phosphorylation and activation. VC orchestrates a dual-defense strategy against ferro-aging: it directly suppresses the pro-aging lipid peroxidation driver ACSL4, while in parallel, it bolsters the cell’s intrinsic antioxidant capacity via Nrf2 pathway activation.
Middle-aged cynomolgus monkeys (12–16 years old, approximating human 40–50 years) received daily oral VC (30 mg/kg group) or a control treatment for 40 months under standardized conditions.
Structural MRI analysis demonstrated that VC intervention counteracted age-related brain atrophy. Using general linear mixed models, we found that VC restored cortical surface area in the frontal lobes of aged monkeys. Regional analysis identified enlargement in four regions of the orbital frontal cortex, an area critical for adaptivebehavior.
Diffusion MRI-based connectomics revealed that, compared with young animals, aged monkeys exhibited reduced structural connectivity in 18 brain regions. VC treatment restored connectivity in 9 of these regions, which were predominantly located in the posterior parietal cortex, a hub for spatial awareness and decision-making.
VC exerted robust neuroprotective effects. It attenuated heterochromatin loss (increased H3K9me3) in the prefrontal cortex and hippocampus and reduced abnormal protein aggregates, including cytosolic aggresomes and Aβ. Additionally, VC lowered the abundance of activated microglia and astrocytes and suppressed expression of the innate immune sensor cGAS in the hippocampus.
VC supplementation reduced the estimated biological age across multiple organs. At the epigenetic level, VC lowered DNA methylation age in several tissues, including brain, brown adipose tissue, muscle, skin, aorta, and kidney. In the hippocampus, the most substantial reductions in biological age occurred in microglia, oligodendroglia, and oligodendrocyte precursor cells. In the pancreas, alpha cells, beta cells, and ductal cells showed the greatest rejuvenation.
In summary, chronic VC supplementation inhibits the ferro-aging pathway, reduces multidimensional biological age across primate organs, and ameliorates a spectrum of functional declines in nervous and metabolic systems. Our work establishes ACSL4 inhibition as a promising and translationally relevant therapeutic strategy for mitigating aging-related decline.
A long-term, 40-month intervention study in aged non-human primates is a highly translational model given their shared inability with humans to synthesize VC endogenously. The finding that a single, safe nutrient can reverse multidimensional aging clocks in a primate has profound implications for translational longevity medicine.”
“For humans (who, like macaques, cannot synthesize vitamin C), the Recommended Dietary Allowance (RDA) is 75–90 mg/day for adults (~1–1.5 mg/kg for a 60–70 kg person) to prevent deficiency. Upper safe intake levels are much higher: up to 2,000 mg/day (Tolerable Upper Intake Level) is considered safe for most adults, with no established adverse effects at that level from food/supplements.
Treated monkeys represent advanced aging stages (likely equivalent to human 50s–70s+ based on ‘aged’ designation and long-term intervention effects), extending the prior 12–16-year monkey range (human ~35–55) to broader anti-aging applications. While human trials are needed, the primate evidence (long-duration, systemic benefits) strengthens the case for high-dose, sustained vitamin C as a strategy against ferro-aging in humans. It elevates vitamin C from a nutrient to a targeted anti-aging compound in primates.”
Coincidentally, I started taking extra vitamin C separately from other supplements in the form of liposomal 1 gram twice daily this past winter. Can’t say that it had any effects on my intended target, avoiding sniffles and sneezing, as allergy season kicked off in early February. With this study’s findings, I’ll continue.
A 2026 rodent study investigated sulforaphane’s ability to affect ALS-like symptoms:
“The objective of this study was to evaluate neuroprotective efficacy and safety of sulforaphane (SUFP) in a methylmercury (MMHg⁺)-induced preclinical rat model of amyotrophic lateral sclerosis (ALS). ALS is characterized by progressive motor neuron degeneration and muscle wasting, leading to impairments in gait, swallowing, salivation, and routine motor activities.
64 animals were classified into eight groups: 1st: normal control, 2nd: vehicle control; 3rd: SUFP perse (4 mg/kg, i.p.), 4th: MMHg + (5 mg/kg, p.o.), 5th: MMHg + 5 + SUFP (2 mg/kg, i.p.), 6th: MMHg+ 5 + SUFP (4 mg/kg, i.p.), 7th: MMHg+ 5 + omaveloxolone (OVX) (30 mg/kg, i.p.), and 8th: MMHg + 5 + dimethyl fumarate (DIMT) (50 mg/kg, i.p.). Neurotoxin MMHg + was orally administered at 5 mg/kg for the first 21 days. For the next 22 days, SUFP, OVX, and DIMT were administered intraperitoneally (i.p.).
SUFP modulates neurotransmitter levels such as acetylcholine (A), dopamine (B), GABA (C), glutamate (D), and serotonin (E).
SUFP4 exerted broad neuroprotective effects in ALS pathology by restoring antioxidant proteins (Nrf2, HO-1, SIRT1), suppressing apoptotic (Bax, caspase-3, Bcl-2) and inflammatory markers (TNF-α, IL-1β), and enhancing the anti-inflammatory cytokine IL-10. It also downregulated stress-related signaling pathways (PI3K/Akt, p75NTRECD, MAPKs) associated with neurodegeneration. These molecular effects translated into meaningful functional recovery, as evidenced by improvements in grip strength, locomotor performance, spatial memory, and depressive-like behavior.
Histopathological evaluation demonstrated attenuation of demyelination and preservation of neuronal architecture including the cerebral cortex, hippocampus, striatum, midbrain, and cerebellum. Beyond central neuroprotection, SUFP exerted systemic benefits by normalizing hepatic enzymes, improving skeletal muscle integrity, restoring redox balance, stabilizing neurofilament and myelin-associated proteins, and correcting hematological alterations.
Despite limitations related to study duration and animal sex, this work strongly positions SUFP as a promising, multi-target therapeutic candidate for ALS with both neural and systemic protective efficacy.”
https://link.springer.com/article/10.1007/s12035-026-05683-5 “Sulforaphane-Mediated Multitarget Therapeutic Effects in Methylmercury-Induced ALS-Like Pathology: Comparative Analysis and Multifaceted Approach to Neuroprotection and Systemic Recovery” (not freely available) Thanks to Dr. Sidharth Mehan for providing a copy.
Unlike A Nrf2 treatment for ALS?, this study didn’t present evidence that its treatment compound was effective for preventing ALS. For one thing, currently-known disease factors involving heat shock proteins and associated genes, some of which are Nrf2 targets, weren’t investigated.
Two Nrf2 activators were used in both studies as comparators of Nrf2 activation effects. Neither omaveloxolone nor dimethyl fumarate are ALS causal treatments, though, and have undesirable side effects.
A human equivalent of this study’s higher sulforaphane dose is ((4 mg x .162) x 70 kg) = 45 mg. 45 mg of sulforaphane might be too much to consistently take at one time because of unpalatability. But I documented taking an estimated 52 mg for a year during 2020-2021 by eating microwaved 3-day-old broccoli sprouts twice a day.
A 2026 review subject was mechanisms and therapeutic potential for Nrf2 activators in combination with mesenchymal stem cells:
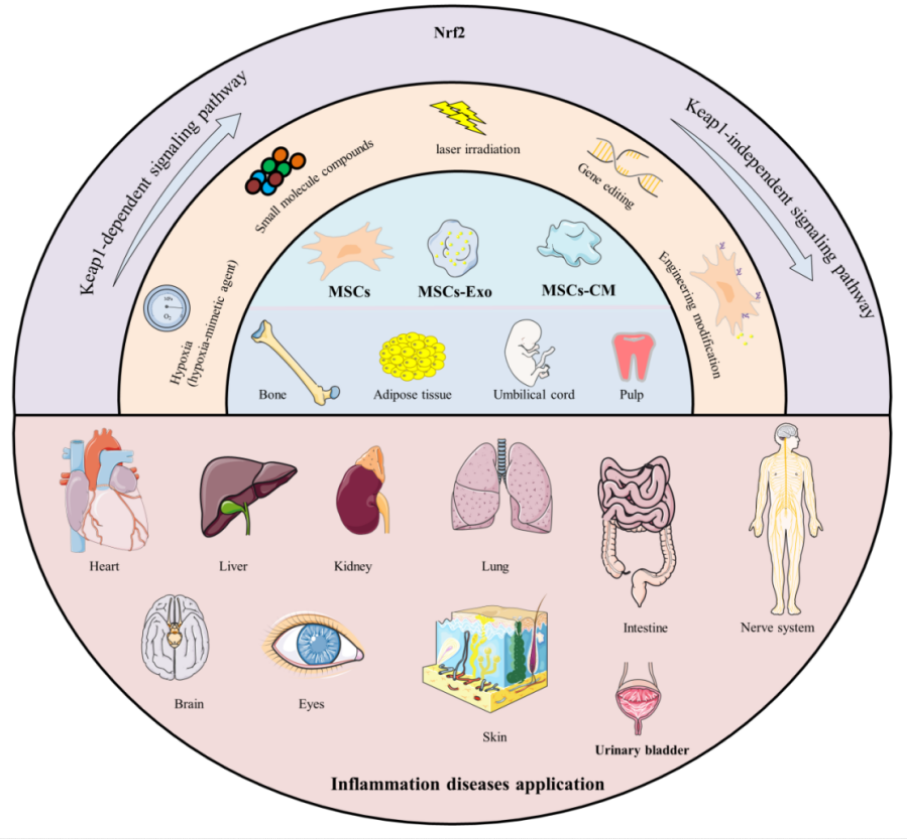
“Mesenchymal stromal/stem cells (MSCs) are multipotent stem cells that can be isolated from various tissues – such as bone marrow (BM), umbilical cord (UC), adipose tissue (AD), dental pulp (DP), hair follicle (HF), and placenta – and differentiated into multiple lineages under appropriate conditions. Their functional repertoire includes immunomodulation, homing, and differentiation, which collectively help establish a balanced inflammatory and regenerative niche within damaged tissues during severe inflammation. MSCs-derived extracellular vesicles (MSCs-EVs) and conditioned medium (MSCs-CM) play remarkable roles, exhibiting potent anti-inflammatory and antioxidant properties that offer novel therapeutic alternatives for inflammatory diseases.
Therapeutic capacity of MSCs in inflammatory conditions is increasingly attributed to their potent paracrine activity rather than solely to their differentiation potential. A key mechanism underlying this paracrine effect is activation of the Nrf2 antioxidant pathway.
MSCs and their secreted products including exosomes (Exos), EVs, and CM, activate Nrf2 through multi-dimensional/target mechanisms, thereby enhancing cellular antioxidant defenses, modulating immune responses, and promoting tissue repair. It is noteworthy that therapeutic efficacy of MSCs and their derivatives can be enhanced through external modulation, including pretreatment with natural compounds.
Preconditioning refers to brief treatment of MSCs or their derivatives with physical, chemical, or biological factors prior to application, aiming to enhance their ability to counteract oxidative stress and improve their therapeutic efficacy. Flavonoids precondition and prime MSCs via the direct Keap1-Nrf2 pathway or indirect PI3K-Akt pathway, which enhances cellular resilience to adverse conditions by reducing apoptosis and promoting survival. Primed MSCs, in turn, remodel the microenvironment through an altered secretory profile, releasing bioactive factors that create more favorable conditions for their own persistence.
The core logic of these strategies lies in simulating or inducing adaptive stress, such as employing specific chemical molecules or drug stimuli, or utilizing physical / microenvironmental preconditioning to mimic specific physical conditions of the in vivo injury environment. The most straightforward strategy is overexpression of Nrf2 or its key downstream effector molecules.
The majority of existing studies remain at the level of observing correlations with Nrf2 upregulation, and there is still a lack of precise causal validation regarding key upstream signals – such as specific cytokines, miRNAs, or proteins – through which MSCs or derivatives initiate Nrf2 activation. Mechanistic insights are predominantly derived from in vivo or rodent (mouse/rat) model experiments, with a notable absence of clinical validation, insufficient long-term safety and pharmacokinetic data, and a lack of standardization in administration routes and dosages, all of which hinder clinical translation.
The essential role of the Nrf2 pathway has not been rigorously confirmed, as most studies have not employed reverse genetic validation using Nrf2-knockout animals or specific inhibitors. Consequently, it remains unclear whether therapeutic effects are necessarily and exclusively dependent on Nrf2, and potential synergistic contributions from other pathways may have been overlooked.
Most natural flavonoids face challenges such as low oral bioavailability, rapid metabolism, and poor targeting. Numerous challenges remain to be addressed in order to translate these promising preclinical findings into clinical practice. Future research should focus on the following aspects:
Elucidating precise upstream molecular mechanisms by which MSCs activate Nrf2;
Employing more clinically relevant chronic disorder models;
Systematically evaluating long-term safety, optimal delivery strategies (including dosage and route of administration), and immunogenicity of MSCs-based therapies;
Validating selection criteria (optimal source), quality control, batch-to-batch consistency of MSCs, and addressing regulatory and ethical barriers to clinical translation; and
Integrating molecular docking, ADMET (Absorption, Distribution, Metabolism, Excretion, Toxicity) prediction, and in vitro and in vivo validation to further elucidate regulatory effects of flavonoids and enhance understanding of their mechanisms of action.”
This paper was overly long at 127 pages, so I focused on the later sections. None of these treatments are currently ready for clinical trials.
I also didn’t mention specific flavonoids as Nrf2 activators. It’s beyond a reviewer’s task to rank Nrf2 activators, and a study’s researchers seldom address why they used a poorly-activating flavonoid instead of a higher-ranked natural plant compound such as sulforaphane.
Here are five 2025 human ergothioneine studies, starting with a clinical trial of healthy older adults:
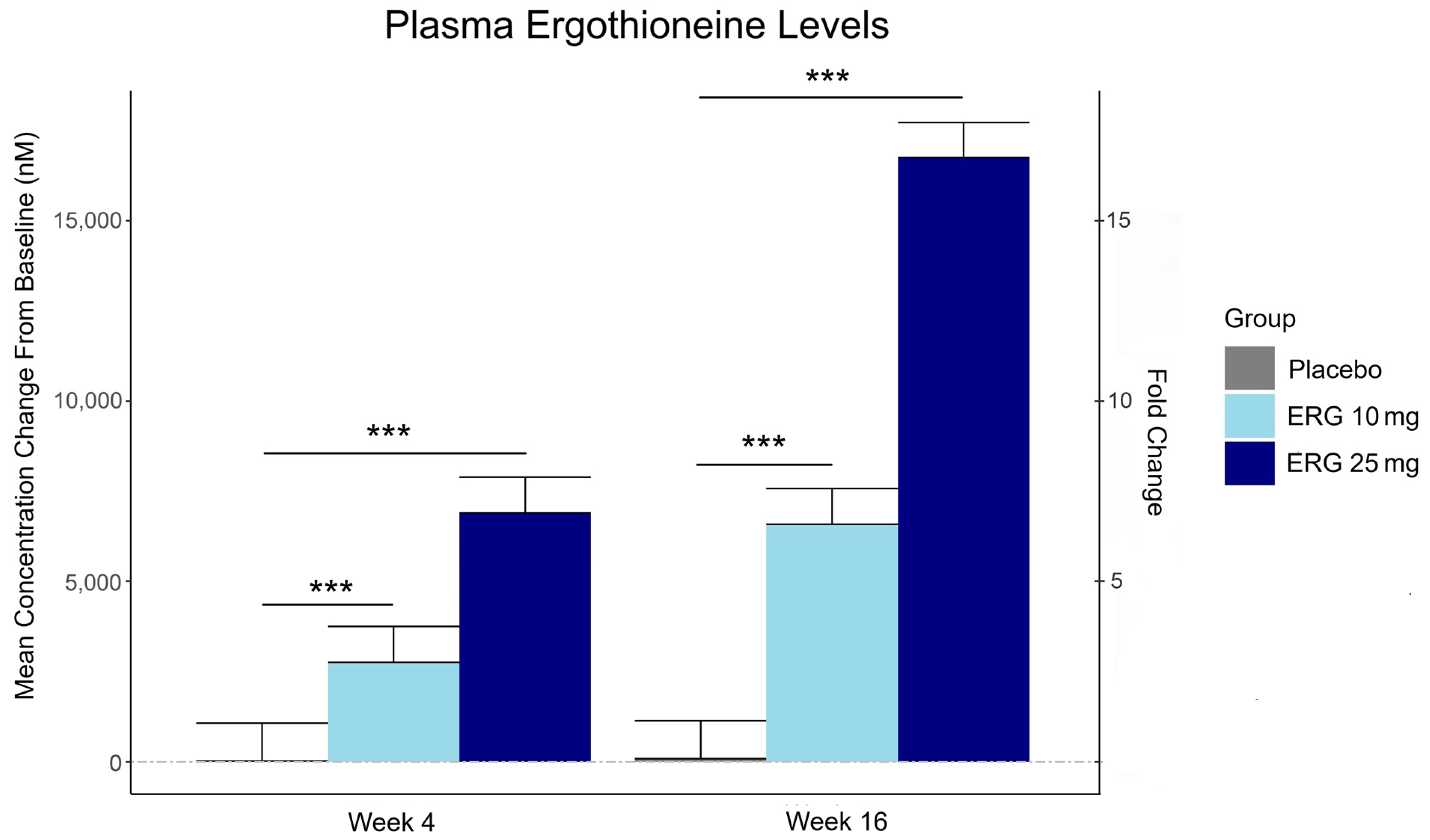
“In this 16-week randomized, double-blind, placebo-controlled trial, 147 adults aged 55–79 with subjective memory complaints received ergothioneine (10 mg or 25 mg/day ErgoActive®) or placebo. Across all the groups, approximately 73% of participants in each group were female, with a median age of 69 years.
The primary outcome was the change in composite memory. Secondary outcomes included other cognitive domains, subjective memory and sleep quality, and blood biomarkers. At baseline, participants showed slightly above-average cognitive function (neurocognitive index median = 105), with plasma ergothioneine levels of median = 1154 nM.
Although not synthesized in the human body, ergothioneine is efficiently absorbed via the OCTN1 transporter (also known as the ergothioneine transporter, or ETT), which is expressed in many tissues, including the intestine, red blood cells, kidneys, bone marrow, immune cells, skin, and brain. This transporter enables ergothioneine to accumulate in high concentrations in organs vulnerable to oxidative stress and inflammation. Ergothioneine has multiple cellular protective functions, including scavenging reactive oxygen species, chelating redox-active metals, suppressing pro-inflammatory signaling, and protecting mitochondrial function.
Plasma ergothioneine increased by ~3- and ~6-fold for 10 mg, and ~6- and ~16-fold for 25 mg, at weeks 4 and 16, respectively.
While the primary outcome, composite memory, showed early improvement in the 25 mg group compared to baseline, this effect was not sustained and did not differ from placebo. Reaction time showed a significant treatment-by-time interaction favoring ergothioneine, yet the between-group differences were not significant, suggesting that any potential benefits were modest and require validation in larger or longer studies.
Other cognitive effects observed were primarily within-group and not consistently dose-responsive, highlighting the challenge of detecting objective cognitive changes over a relatively short study duration in high-functioning healthy populations. However, positive effects of ergothioneine supplementation were observed on subjective measures of prospective memory and sleep initiation that were not seen in the placebo group.
This trial adds to the growing body of evidence supporting the favorable safety profile of ergothioneine. No adverse events attributable to ergothioneine were reported. Additionally, we observed potential hepatoprotective effects, with significant reductions in the plasma AST and ALT levels, particularly among males in the ERG 25 mg group.”
https://www.mdpi.com/1661-3821/5/3/15 “The Effect of Ergothioneine Supplementation on Cognitive Function, Memory, and Sleep in Older Adults with Subjective Memory Complaints: A Randomized Placebo-Controlled Trial”
The third graphic for Ergothioneine dosing, Part 2 showed a human study where a 25 mg dosing stopped after Day 7, but the plasma ergothioneine level stayed significantly higher than baseline through Day 35.
The second graphic for Ergothioneine dosing, Part 2 was a male mouse experiment where plasma ergothioneine levels of a human equivalent 22 mg to 28 mg daily dose kept rising through 92 weeks.
This trial couldn’t explain the desirability of a 25 mg daily dose that was likely (per the second and third graphics for Ergothioneine dosing, Part 2) to sustain the subjects’ increased plasma ergothioneine levels well after the trial ended at Week 16. What effects can be expected from a sustained plasma ergothioneine level that’s 16 times higher than the subjects’ initial levels? Were these 16-fold sustained plasma ergothioneine levels better or worse than the 6-fold increases in the 10 mg group, both of which were likely to continue past the trial’s end?
A representative of the trial’s sponsoring company talked a little more about the trial in this interview:
Another clinical trial investigated ergothioneine’s effects on skin:
“We conducted an 8-week, randomized, double-blind, placebo-controlled clinical trial to evaluate effects of daily oral supplementation with 30 mg of ergothioneine (DR.ERGO®) on skin parameters in healthy adult women aged 35–59 years who reported subjective signs of skin aging. Objective measurements including melanin and erythema indices, skin glossiness, elasticity, and wrinkle and pigmentation counts were used to comprehensively evaluate changes in skin condition.
The OCTN1 transporter is preferentially expressed in basal and granular epidermal layers, where cellular renewal and barrier maintenance are most active. Once internalized, ergothioneine localizes to mitochondria, where it directly scavenges reactive oxygen species (ROS) and protects mitochondrial DNA from UV- and inflammation-induced damage.
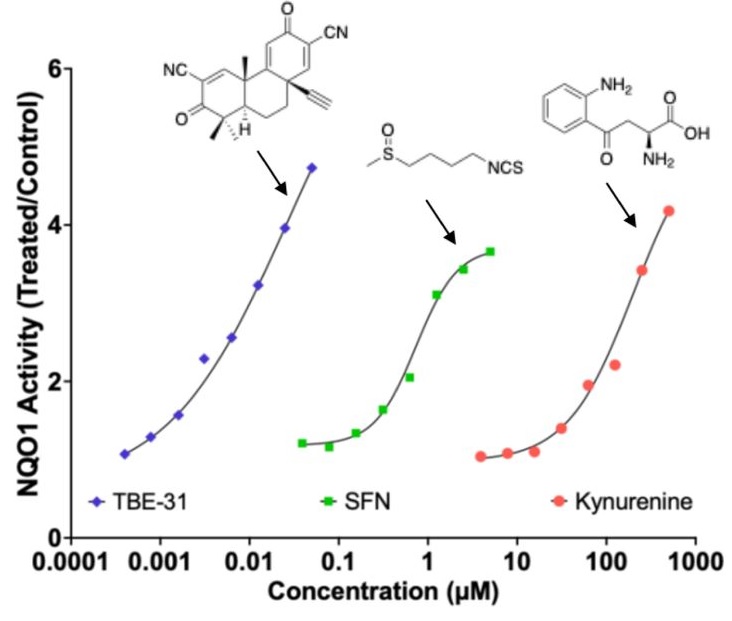
At the signaling level, ergothioneine activates key protective pathways such as the Nrf2/ARE axis, enhancing expression of antioxidant enzymes including HO-1, NQO1, and γ-GCLC. These enzymes contribute to redox homeostasis and glutathione regeneration, reinforcing cellular defense systems against photoaging and environmental insult.
In parallel, ergothioneine modulates the PI3K/Akt/Nrf2 and SIRT1/Nrf2 pathways, which are implicated in collagen preservation, inflammation resolution, and mitochondrial maintenance. These pathways converge to reduce matrix metalloproteinase (MMP) activity, enhance collagen synthesis, and suppress pro-inflammatory cytokines (TNF-α, IL-6, IL-1β), all of which are central to maintaining skin structure and function.
Compared to placebo, the DR.ERGO® ergothioneine group showed significantly greater improvements in melanin and erythema reduction, skin glossiness, elasticity, and wrinkle and spot reduction. No adverse events were reported.
These findings corroborate and extend previous clinical evidence from (Hanayama et al., 2024), who investigated an ergothioneine-rich mushroom extract (Pleurotus sp., 25 mg ergothioneine/day) in a 12-week randomized double-blind trial, and (Chunyue Zhang, 2023), who examined pure ergothioneine supplementation (25 mg/day) in a 4-week open-label study. We contextualized our results within this existing literature by comparing key outcomes.
Several limitations should be acknowledged:
The study cohort consisted solely of Japanese women aged 35–59 years, which may limit generalizability across sexes, ethnicities, and age groups.
The 8-week intervention period, while sufficient to detect short-term effects, does not allow conclusions about the sustainability of benefits or the risk of relapse upon discontinuation.
The placebo group also showed modest improvements in self-perception, highlighting the well-documented placebo response in beauty and wellness studies.
This study focused on a single daily dosage (30 mg/day) without evaluating dose–response relationships, and hydration-specific endpoints such as corneometry or transepidermal water loss (TEWL) were not included.”
Two clinical trials investigated ergothioneine’s effects on sleep quality:
“A four-week administration of 20 mg/day ergothioneine (EGT), a strong antioxidant, improves sleep quality; however, its effect at lower doses remains unclear. This study estimated the lower effective doses of EGT using a physiologically based pharmacokinetic (PBPK) model in two clinical trials.
In Study 1, participants received 5 or 10 mg/day of EGT for 8 weeks, and their plasma and blood EGT concentrations were measured. An optimized PBPK model incorporating absorption, distribution, and excretion was assembled. Our results showed that 8 mg/day of EGT for 16 weeks was optimal for attaining an effective plasma EGT concentration.
In Study 2, a randomized, double-blind, placebo-controlled study, participants received 8 mg/day EGT or a placebo for 16 weeks. The subjective sleep quality was significantly improved in the EGT group than in the placebo group.
In mammals, EGT is not generated in the body but is acquired from the diet via the carnitine/organic cation transporter OCTN1/SLC22A4. Its plasma concentration after oral administration is quite stable and gradually increases after repeated dosing on a multi-day basis.
Blood concentrations of EGT increase after Day 8 when EGT intake is interrupted, and they continue to increase until Day 35. The delayed increase in EGT concentration in the blood, compared with that in the plasma, can be interpreted as its efficient uptake by undifferentiated blood cells, which express high levels of OCTN1/SLC22A4 in the bone marrow, and subsequent differentiation to mature blood cells that enter the circulation. This may imply the nonlinear absorption, distribution, and excretion of EGT owing to saturation of the transporter at higher concentrations, potentially leading to difficulty in model construction.
This is the first study to propose a strategy to estimate lower effective doses based on the PBPK model.”
The bolded section above referenced a 2016 study / third graphic for Ergothioneine dosing, Part 2, where a 25 mg dosing stopped after Day 7, but the plasma ergothioneine level stayed high through Day 35. I didn’t see that the referenced 2004 and 2010 studies addressed this 2016 finding.
I also didn’t see that this study’s mathematical model accounted for saturation of the OCTN1 transporter or other effects, such as a very small ergothioneine clearance rate. Okay, lower the ergothioneine dose, and achieve a lower persistent plasma ergothioneine level, to what benefit?
“The present study demonstrated that OCTN1 is associated with myeloid cells rather than lymphoid cells, and especially with erythroid-lineage cells at the transition stage from immature erythroid cells to peripheral mature erythrocytes.”
Persistent high ergothioneine levels aren’t costless. Skewing bone marrow stem cells and progenitor cells toward a myeloid lineage is done at the expense of lymphocytes, T cells, B cells, and other lymphoid lineages.
Where are the studies that examine these tradeoffs? Subjective sleep quality in this study and sleep initiation in the first study above aren’t sufficiently explanatory.
A study investigated associations of plasma ergothioneine levels and cognitive changes in older adults over a two-year period:
“Observational studies have found that lower plasma levels of ergothioneine (ET) are significantly associated with higher risks of neurodegenerative diseases. However, several knowledge gaps remain:
Most of the above studies were based on cross-sectional study design, and potential reverse causation cannot be excluded. It has been suggested that plasma ET declines concomitantly with the deterioration of cognitive function.
Since the impact of a single dietary factor on health is mild, it is prone to be affected by the baseline characteristics of subjects (such as sex, educational level, disease status and gene polymorphism). However, no study has systematically evaluated potential effect modifiers on the association between ET levels and cognitive function.
The dose-response distribution between ET and cognitive function remains undetermined.
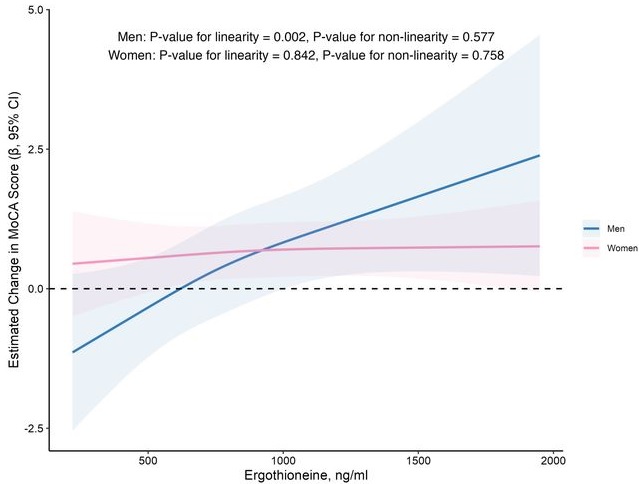
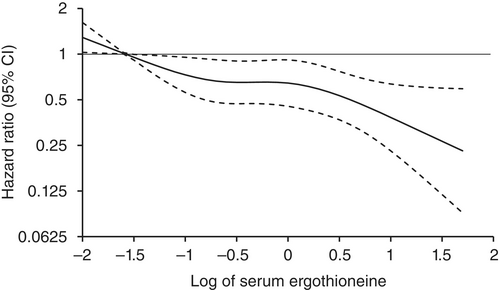
In this prospective cohort study of 1,131 community-dwelling older adults (mean age 69 years), higher baseline plasma ET levels were significantly associated with slower cognitive decline, as assessed by Montreal Cognitive Assessment (MoCA) scores, during a 2-year follow-up period.
When the plasma concentration of ET exceeds 1,000 ng/mL, the decline in cognitive function significantly slows down. However, this association has only been observed in men.
Domain-specific analysis found that the observed ET-MoCA association was mainly driven by the temporary slowdown in the decline of visuospatial/executive and delayed recall. Impaired delayed recall represents one of the earliest and most sensitive cognitive markers of dementia progression, predictive of conversion from MCI to dementia. The preferential preservation of this function by ET suggests targeted neuroprotective effects within the hippocampus.
Visual inspection of the spline curves revealed a potential plateauing effect at ET concentrations ≥1,000 ng/mL in the total population.
Baseline ET concentrations differed between men and women. Most men (81.5%) had concentrations below 1,000 ng/mL (median 754.2, IQR 592.0–937.9 ng/mL). Women exhibited substantially higher median plasma ET concentrations than men, with 35.7% of women exceeded 1,000 ng/mL (median 890.1, IQR 709.7–1,095.6 ng/mL).
Our study included only participants with normal cognitive function, and the results remained robust even after excluding those with baseline cognitive function at the lower end of the normal range. Collectively, our findings support that low ET intake occurs prior to cognitive decline.
Our findings indicate that higher plasma ET levels are significantly associated with slower cognitive decline independent of confounders in non-demented community-dwelling elderly participants, with such association observed in men but not women. Dose-response curves indicated plateauing effects above 1000 ng/mL.”
The average age of this study and the first trial above were both 69 years. Since the first trial’s participants showed slightly above-average cognitive function (neurocognitive index median = 105), with plasma ergothioneine levels of median = 1154 nM at baseline, and this study showed plateauing effects above 1000 ng/mL, I wonder how raising plasma ergothioneine levels above 1000 ng/mL could possibly show a net benefit for older people? What are the trade-offs for older people between potentially increasing slightly above-average cognitive function with ergothioneine and its other effects from saturating their OCTN1 transporter?
This study is at its preprint stage. I’m interested to see if its peer review prompts these researchers to also investigate the common finding that people who are most deficient at baseline have the greatest improvements. If so, would these sex-specific associations still hold?
Wrapping up with a study that investigated associations of serum ergothioneine levels with the risk of developing dementia:
“1344 Japanese community-residents aged 65 years and over, comprising 765 women and 579 men, without dementia at baseline were followed prospectively for a median of 11.2 years.
During follow-up, 273 participants developed all-cause dementia. Among them, 201 had Alzheimer’s disease (AD) and 72 had non-Alzheimer’s disease (non-AD) dementia.
Age- and sex-adjusted hazard ratios (HRs) for all-cause dementia, AD, and non-AD dementia decreased progressively across increasing quartiles of serum ergothioneine. These associations remained significant after adjustment for a wide range of cardiovascular, lifestyle, and dietary factors, including daily vegetable intake.
In subgroup analysis, association between serum ergothioneine levels and the risk of dementia tended to be weaker in older participants and in women:
In older individuals, cumulative burden of multiple risk factors such as hypertension, diabetes mellitus, and smoking may contribute to both neurodegenerative and vascular pathology, potentially diminishing the relative influence of ergothioneine.
In women, postmenopausal hormonal changes, particularly the decline in estrogen, have been associated with increased oxidative stress and a higher vulnerability to neurodegenerative changes.
Several limitations should be noted:
Since serum ergothioneine levels and other risk factors were measured only at baseline, we could not evaluate the changes of serum ergothioneine levels during the follow-up period. Lifestyle modifications during follow-up could have influenced serum ergothioneine levels and other risk factors. In addition, serum ergothioneine level was measured only once, and from a sample.
We cannot rule out residual confounding factors, such as other nutrients in mushrooms and socioeconomic status.
There is a possibility that dementia cases at the prodromal stage were included among participants with low serum ergothioneine levels at baseline.
We are unable to specify which mushroom varieties were predominantly consumed by participants in the town of Hisayama.
Given the limited discriminative ability of serum ergothioneine and potential degradation due to long-term sample storage, we were unable to explore a clinically meaningful threshold value of serum ergothioneine.
Generalizability of findings was limited because participants of this study were recruited from one town in Japan.
These findings suggest that the potential benefit of ergothioneine may be attenuated in individuals with pre-existing, multifactorial risk profiles for dementia.
Our findings showed that higher serum ergothioneine levels were associated with a lower risk of developing all-cause dementia, AD, and non-AD dementia in an older Japanese population. Since ergothioneine cannot be synthesized in the human body, a diet rich in ergothioneine may be beneficial in reducing the risk of dementia.”
For five years I got most of my estimated 7 mg daily ergothioneine intake from mushrooms in AGE-less chicken vegetable soup per Ergothioneine dosing. The soup was always boring, but I got too bored this year and stopped making it. I haven’t replaced mushroom intake with supplements.
I still don’t eat fried or baked foods, preferring sous vide and braising cooking methods to avoid exogenous advanced glycation end products. I avoid buying foods that evoke a hyperglycemic response or otherwise form excessive endogenous AGEs per All about AGEs.
Here are two 2025 papers, starting with a rodent study that investigated interactions between the Nrf2 and kynurenine pathways:
“Exposure to the tryptophan metabolite kynurenine and its electrophilic derivative kynurenine-carboxyketoalkene (Kyn-CKA) leads to an increase in the abundance of transcription factor Nrf2 and induction of Nrf2-target genes. The Keap1/Nrf2 system is the main orchestrator of cellular defence against environmental stress, most notably oxidative and inflammatory stress.
Nrf2 can be activated pharmacologically by small molecules, the majority of which are electrophiles and oxidants that modify specific cysteine-based sensors in Keap1. C151 in Keap1 is the target of the isothiocyanate sulforaphane, a classical Nrf2 activator that has been employed in ∼90 clinical trials, as well as for the two Nrf2 activators that are clinically in use: dimethyl fumarate, for relapsing remitting multiple sclerosis, and omaveloxolone, for Friedreich’s ataxia.
Kynurenine is an endogenous metabolite derived from the essential amino acid tryptophan. Kynurenine and its metabolites, such as the electrophilic kynurenine-carboxyketoalkene (Kyn-CKA), have been demonstrated to activate Nrf2 in other pathologies, including sickle cell disease, attenuating inflammation. Moreover, identification of the gene encoding the kynurenine-metabolising enzyme kynureninase as a gene transcriptionally upregulated by Nrf2, provides a plausible negative feedback regulatory mechanism.
Because kynurenine is not electrophilic, whereas its metabolite Kyn-CKA is, we considered the possibility that Kyn-CKA is the actual Nrf2 activator. Using biochemical and cell-based assays, we found that Kyn-CKA reacts with C151 in the BTB domain of Keap1 and increases the thermostability of Keap1, indicating target engagement. Consequently, Nrf2 accumulates and induces transcription of antioxidant/electrophile-responsive element (ARE/EpRE)-driven genes.
These findings demonstrate that Kyn-CKA targets C151 in Keap1 to derepress Nrf2, and reveal that Nrf2 is a main contributor to the anti-inflammatory activity of Kyn-CKA in macrophages.”
A review subject was targeting nicotinamide adenine dinucleotide, oxidized form (NAD+) for clinical use:
“Mammalian NAD+ biosynthesis includes four known pathways, primarily occurring in cytoplasm:
(a) the NRH pathway;
(b) the salvage pathway;
(c) the Preiss–Handler pathway; and
(d) the kynurenine pathway.
The de novo kynurenine pathway metabolizes tryptophan (Trp) to NAD+, producing various intermediates that serve as biomarkers for different diseases. These intermediates show alterations in various pathological conditions.
While kynurenine and its metabolic derivatives are intermediates in the de novo NAD+ biosynthesis pathway, these are also produced independently in various physiological contexts, particularly in immune cells, where they act as immunomodulatory compounds.”
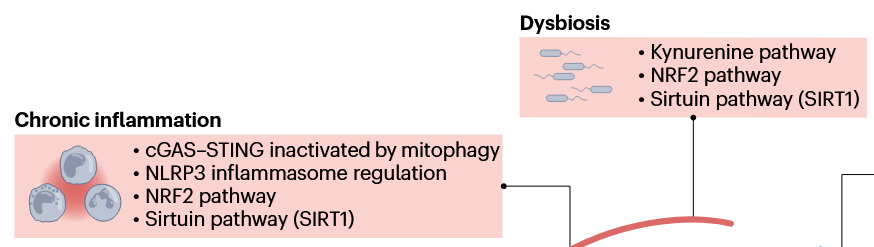
This second paper above showed a graphic of the Nrf2 and kynurenine pathways together in a diagram showing relationships between NAD+ augmentation and the hallmarks of aging, but didn’t elaborate other than labeling their box Dysbiosis. So how these two pathways interact is better outlined in the first paper above with explaining how a kynurenine-metabolizing enzyme is one of the hundreds of Nrf2 target genes, creating a natural feedback loop between Nrf2 activation and the kynurenine pathway.
These reviewers also lumped SIRT1 in their Dysbiosis box, and into several other boxes, probably due to the penultimate coauthor’s influence:
However, repeating something over and over doesn’t make it scientifically valid regardless of the number of citations. Or, as a 2022 review Sirtuins are not conserved longevity genes concluded:
“A global pursuit of longevity phenotypes was driven by a mixture of framing bias, confirmation bias, and hype. Review articles that propagate these biases are so rampant that few investigators have considered how weak the case ever was for sirtuins as longevity genes.
Acknowledging that a few positive associations between sirtuins and longevity have been identified after thousands of person-years and billions of dollars of effort, we review the data and suggest rejection of the notions that sirtuins (i) have any specific connection to lifespan in animals and (ii) are primary mediators of the beneficial effects of NAD repletion.”
Continuing Plasmalogens Week with two 2025 papers, starting with a rodent study of plasmalogens’ effects on mitigating cognitive decline:
“We evaluated beneficial effects of plasmalogens (PLS), phosphatidylcholine (PC), and phosphatidylserine (PS) on age-associated cognitive decline. We established a mouse model of aging-associated cognitive impairment using the subcutaneous injection of d-galactose (D-gal) at a dosage of 400 mg/kg/day.
We randomly divided six-week-old female mice into nine groups: control, model, high-dose PLS (0.3 mg/kg/day), low-dose PLS (0.09 mg/kg/day), high-dose PC (200 mg/kg/day), low-dose PC (50 mg/kg/day), high-dose PS (200 mg/kg/day), low-dose PS (50 mg/kg/day), AMC-Plas (120 mg/kg/day; and functional component PLS (0.252 mg/kg/day).
We administered PLS, PC, and PS separately by oral gavage once daily. We extracted PLS from scallops according to the literature. AMC-Plas is a commercially available health supplement known for its neuroprotective properties and memory-enhancing effects. In this study, we included AMC-Plas as a positive control group to evaluate the effects of different phospholipids.
Synaptophysin (SYP), synapsin-1 (SYN-1), postsynaptic density protein 95 (PSD-95), and brain-derived neurotrophic factor (BDNF) play important roles in synapse formation and synaptic plasticity. Synaptic function alterations or losses are key pathological mechanisms that underlie development of cognitive impairment. Therapeutic strategies that attempt to restore synaptic function or promote synaptic remodeling are considered to be increasingly promising strategies to mitigate cognitive decline.
Results showed that:
PLS improved spatial memory performance by 44% and object recognition by 80% in D-galactose-induced cognitively impaired mice.
PLS significantly decreased glial fibrillary acidic protein (GFAP)-positive cells (an indicator of astrocyte activation) in the dentate gyrus (DG) of the hippocampus, an important result because the DG is a crucial neurogenesis region.
PLS alleviated neuronal damage and protected against synaptic injury, verified by a 228% increase in PSD-95 expression in the hippocampus.
PLS showed a more prominent role for the mitigation of age-related cognitive impairment compared with PC and PS.
In conclusion, the evaluation of PLS using both behavioral and neuropathological assessments in cognitively impaired mice highlighted its exceptional efficacy compared with other phospholipids. PLS at a remarkably low effective dose significantly ameliorated cognitive deficits in cognitively impaired mice. This result further emphasized its potential relevance in neurodegenerative disease research.
We found that PLS alleviated cognitive impairment potentially by improving synaptic function; however, the molecular mechanisms that underlie its effects on synaptic function warrant further investigation.”
There was no disclosed chemical analysis of the PLS scallop extract’s plasmalogen types or other contents. Despite its name, I didn’t see that the AMC-Plas product contained plasmalogens or plasmalogen precursors.
A fruit fly study investigated plasmalogen effects on mitochondria during aging:
“We identify plasmalogens—endogenous ether-linked phospholipids—as key regulators of age-associated mitochondrial fission in Drosophila melanogaster. Loss of Kua (also known as plasmanylethanolamine desaturase (PEDS) / TMEM189 in mammals), the enzyme essential for plasmalogen biosynthesis, leads to inhibition of mitochondrial fission and impaired recruitment of the fission protein Drp1, similar to what is observed during aging.
Mitochondrial dynamics, comprising balanced cycles of fission and fusion, are essential for preserving organelle quality, metabolic flexibility, and cellular homeostasis throughout life. Aging disrupts this balance, with multiple studies reporting a decline in mitochondrial fission that contributes to the accumulation of enlarged and dysfunctional mitochondria.
These morphological changes are linked to impaired mitophagy, altered energy production, and tissue dysfunction. Midlife induction of Drp1—the dynamin-related GTPase that drives mitochondrial division—has been shown to reverse age-related mitochondrial defects and prolong lifespan in Drosophila.
To determine whether plasmalogen biosynthesis is essential for mitochondrial fission, we used KuaMI04999, a hypomorphic allele. Western blot analysis revealed significantly reduced Kua protein levels in KuaMI04999/+ heterozygotes compared to wild-type controls.
Our findings reveal a previously unrecognized lipid-based mechanism that controls mitochondrial fission during aging and position plasmalogens as key effectors linking membrane composition to mitochondrial homeostasis. It is not merely expression or stability of Drp1 that is affected, but rather its recruitment to the mitochondrial surface, which is a critical activation step for fission.
While our study highlights the requirement of plasmalogen biosynthesis for Drp1 recruitment, further work is needed to understand how plasmalogens mechanistically facilitate this interaction.”
A 2025 rodent study investigated mechanisms by which erythropoietin (EPO) enables adult neurogenesis and cognitive function:
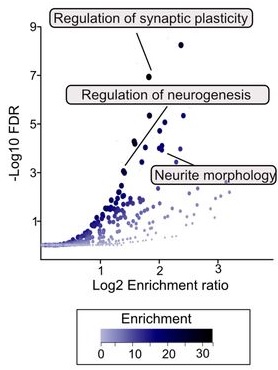
“We mapped epigenomic and transcriptional landscapes of adult mouse hippocampus under recombinant human EPO (rhEPO) treatment. We discovered significant lineage-specific remodelling of chromatin accessibility predominantly in newly formed pyramidal neurons, highlighting a robust EPO-driven neurogenic response. Notably, transposable elements (TEs), particularly ancient LINEs and SINEs, emerged as critical cis-regulatory elements (cCREs).
EPO is known to be upregulated in the brain under hypoxic or injury conditions, and it has been considered a natural neuroprotective agent. We demonstrated that EPO, a traditionally hematopoietic hormone, can profoundly reprogram the adult neural epigenome to drive neurogenesis.
EPO may activate a specific subclass of dormant regulatory elements to drive nearby genes. Such a mechanism would represent a previously unappreciated mode of gene regulation: the de novo recruitment of ancient genomic elements to drive a contemporary cellular response.
Our data support the model that EPO drives differentiation of progenitors rather than inducing widespread cell division. The net effect is an enrichment of pyramidal neurons at the cost of interneurons. Pyramidal neurons integrate in the hippocampal circuitry, leading to potential implications for mood, memory, cognitive enhancement, and recovery from brain injury.
We propose a conserved evolutionary mechanism at play: ancient TEs embedded in the genome have been repurposed as cCREs in neural cells, and during an EPO-induced neurogenic stimulus, the brain taps into this reservoir of regulatory elements to rapidly reshape gene expression. In evolutionary terms, this represents an efficient strategy.”
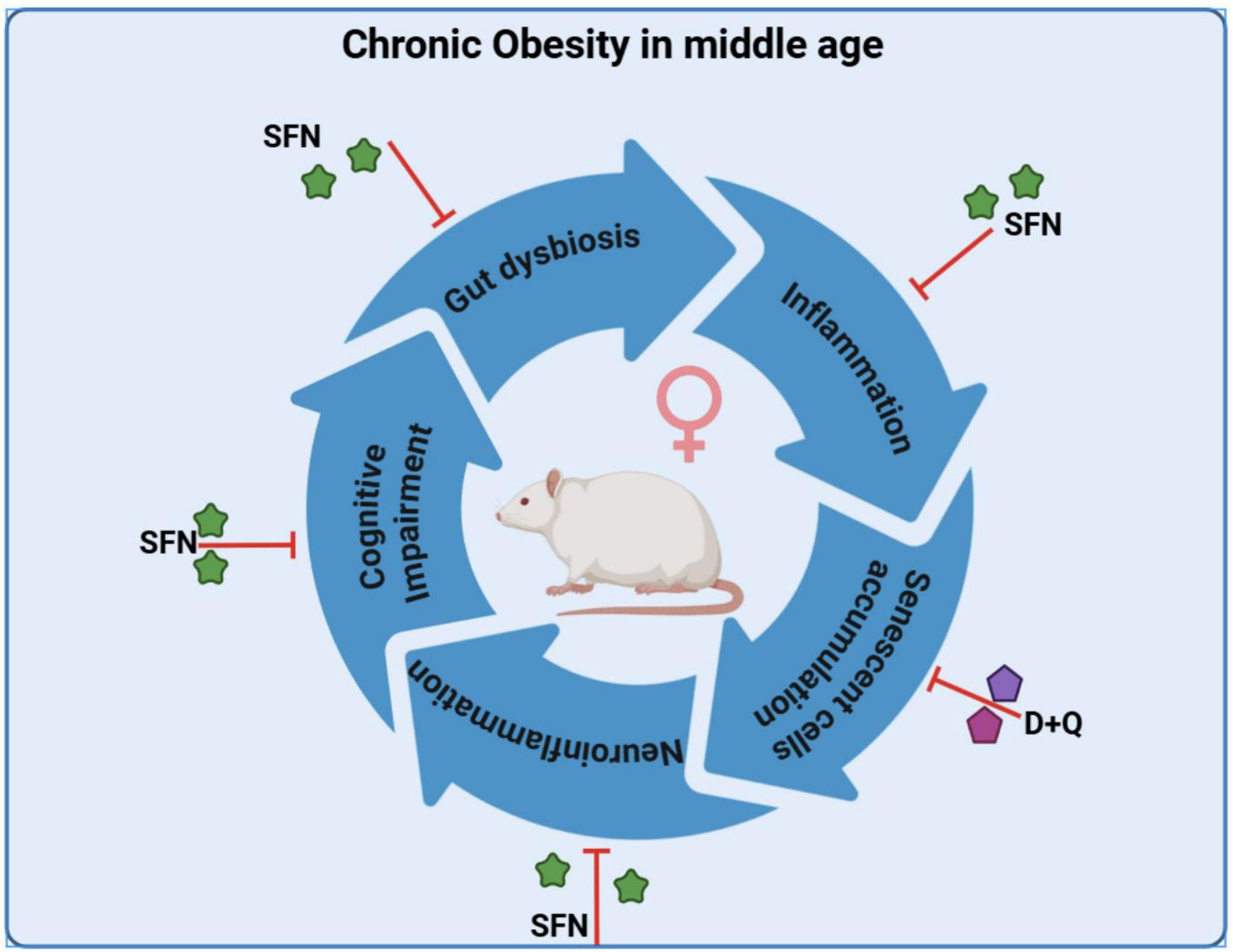
A 2025 rodent study by the same group as Part 1 investigated similar subjects from a different experimental angle of senotherapy effects on brain and behavior rather than cardioprotective effects of dasatinib / quercetin (a senolytic combination) and sulforaphane (senomorphic):
“This is the first study to analyze the effect of senotherapy in the brain of a model of chronic obesity in middle-aged female rats. D + Q reduced the pro-inflammatory cytokines evaluated in the obesity model. It did not improve memory and learning nor the expression of molecules associated with the maintenance of synapses.
In contrast, sulforaphane (SFN), which without eliminating senescent cells, decreased pro-inflammatory factors, increased IL-10, as well as brain-derived neurotrophic factor BDNF, synaptophysin (SYP), and postsynaptic density protein 95 (PSD-95), which, in turn, were associated with an improvement in behavioral tests in obese rats. This suggests that modulating the senescence-associated secretory phenotype (SASP), rather than eliminating senescent cells, might have better effects.”
A 2025 rodent study investigated effects of far-infrared light on Alzheimer’s disease models. I’ll focus on its Nrf2 findings:
“Far-infrared radiation (FIR) is commonly utilized as a complementary treatment of a range of disease, for example, insomnia and rheumatoid arthritis. In this research, we explored how FIR light impacts cognitive functions of TgCRND8 AD mice and elucidated its underlying molecular mechanism.
Infrared radiation is a form of electromagnetic energy that has wavelengths between 750 nm and 1000 μm, which are longer than visible light. International Commission on Illumination categorizes infrared light as three sub-divisions according to the wavelength: (1) near-infrared radiation (0.7–1.4 μm), (2) middle infrared radiation (1.4–3.0 μm), and (3) far-infrared radiation (3.0–1000 μm).
Nrf-2/ HO-1 signaling, a key endogenous antioxidant system, helps mitigate oxidative stress and enhances expression of various endogenous genes. Activation of HO-1 during inflammatory conditions may serve as an adaptiveresponse to reduce cytotoxicity through various mechanisms.
In this study, we applied EFFIT LITE® as the FIR spectrum transmitter which stably radiates an FIR spectrum with a wavelength of 4–20 μm, and the device was put within 1 cm directly above the head of the 3-month-old TgCRND8 mice for 30 min exposure once every day. FIR light notably enhanced cognitive function and spatial memory of TgCRND8 mice after 28-days consecutive treatment.
Underlying molecular mechanisms involve suppression of Aβ deposition, hyperphosphorylation of tau, and neuroinflammation through modulating Jak-2/Stat3 and Nrf-2/HO-1 pathways. Our current experimental findings amply indicate that FIR light is a potential non-pharmacological therapy for AD.”
This study measured Nrf2 and its quickly-induced downstream enzyme HO-1 effects of daily far-infrared light exposure for 30 minutes. We’d have to see measurements of Nrf2’s more-slowly induced and longer-lasting downstream xenobiotic detoxifying enzyme NQO1 to compare far-infrared light Nrf2 activation effects with those of natural plant compounds.
“AMD progression from intermediate to late AMD leads to a point of irreversible retinal pigmented epithelium (RPE) degeneration where treatment becomes worthless. Treating patients at the early/intermediate stages presents a better therapeutic window opportunity for AMD as the disease could potentially be prevented or slowed down.
Strong evidence points to RPE dysfunction at these stages, mainly through redox imbalance and lysosomal dysfunction in RPE oxidative injury. Restoring oxidative balance and lysosomal function may act as preventive and therapeutic measures against RPE dysfunction and degeneration.
Due to interaction with KEAP1, NRF2 is a ubiquitously expressed protein with a high turnover and half-life of about 20 minutes. Because the turnover of NRF2 is faster than KEAP1, newly synthesized NRF2 does not have free KEAP1 to bind and is translocated into the nucleus. Once in the nucleus, NRF2 dimerizes with sMAF and the complex binds to antioxidant response element (ARE) sequences, promoting the expression of ARE genes.
There is NRF2 involvement in most of the hallmarks of aging. Key transcriptional regulatory factors of related pathways, such as transcription factor EB (TFEB) and NRF2, may be targeted to restore homeostasis and/or prevent further RPE degeneration.”
There were other informative tidbits throughout this review, such as:
“Anti-inflammatory effects of most electrophilic NRF2 activators are thought to be at least partly NRF2-independent, suggesting that these compounds lacking specificity may be advantageous for multitargeted pathologies.
TFEB can activate NRF2 under conditions devoid of oxidative stress.”
In this human cell and rodent study, several coauthors of the original 2020 study tested sulforaphane and TFEB interactions for ameliorating effects of a rare disease:
“Mutations in genes encoding lysosomal proteins could result in more than approximately 70 different lysosomal storage disorders. Niemann–Pick disease type C (NPC) is a rare lysosomal storage disorder caused by mutation in either NPC1 or NPC2 gene. Deficiency in NPC1 or NPC2 protein results in late endosomal/lysosomal accumulation of unesterified cholesterol.
Clinical symptoms of NPC include hepatosplenomegaly, progressive neurodegeneration, and central nervous system dysfunction, that is, seizure, motor impairment, and decline of intellectual function. So far there is no FDA-approved specific therapy for NPC.
Under stress conditions, that is, starvation or oxidative stress, TFEB is dephosphorylated and actively translocates into the nucleus, promoting expression of genes associated with lysosome and autophagy. TFEB overexpression or activation results in increased number of lysosomes, autophagy flux, and exocytosis.
Pharmacological activation of TFEB by sulforaphane (SFN), a previously identified TFEB agonist, significantly promoted cholesterol clearance in human and mouse NPC cells, while genetic inhibition (KO) of TFEB blocked SFN-induced cholesterol clearance. This clearance effect exerted by SFN was associated with upregulated lysosomal exocytosis and biogenesis. SFN treatment has no effect on the liver and spleen enlargement of Npc1 mice.
SFN is reportedly BBB-permeable, assuring a good candidate for efficient delivery to the brain, which is essential for targeting neurodegenerative phenotypes in neurological diseases including NPC. This is the first time that SFN was shown to directly activate TFEB in the brain.
Collectively, our results demonstrated that pharmacological activation of TFEB by a small-molecule agonist can mitigate NPC neuropathological symptoms in vivo. TFEB may be a putative target for NPC treatment, and manipulating lysosomal function via small-molecule TFEB agonists may have broad therapeutic potential for NPC.”
https://elifesciences.org/articles/103137 “Small-molecule activation of TFEB alleviates Niemann–Pick disease type C via promoting lysosomal exocytosis and biogenesis”
A 2025 review subject was sulforaphane and brain health. This paper was the latest in a sequence where the retired lead author self-aggrandized his career by citing previous research.
He apparently doesn’t personally do what these research findings suggest people do. The lead author is a few weeks older than I am, and has completely white hair per an interview (Week 34 comments). I’ve had dark hair growing in (last week a barber said my dark hair was 90%) since Week 8 of eating broccoli sprouts every day, which is a side effect of ameliorating system-wide inflammation and oxidative stress.
If the lead author followed up with what his research investigated, he’d have dark hair, too. Unpigmented white hair and colored hair are both results of epigenetics.
Contrast this lack of personal follow-through of research findings with Dr. Goodenowe’s protocol where he compared extremely detailed personal brain measurements at 17 months and again at 31 months. He believes enough in his research findings to personally act on them, and demonstrate to others how personal agency can enhance a person’s life.
It’s every human’s choice whether or not we take responsibility for our own one precious life. I’ve read and curated on this blog many of this paper’s references. Five years ago for example:
I haven’t mentioned α-ketoglutarate for a while, although I’ve taken it twice a day for several years. Here are four 2025 papers on α-ketoglutarate, starting with a review of its role in bone health:
“α-Ketoglutarate (α-KG) serves as a pivotal intermediate in various metabolic pathways in mammals, significantly contributing to cellular energy metabolism, amino acid metabolism, and other physiological processes. α-KG may be a therapeutic target for a variety of bone-related diseases, such as osteoporosis, osteoarthritis, and rheumatoid arthritis, because of its role in maintaining metabolic balance of bone.
α-KG, as a rate-determining mitochondrial intermediate, is crucial in cell energy metabolism because it connects intracellular carbon and nitrogen metabolism between isocitrate and succinyl coenzyme A. Additionally, α-KG is closely involved in the amino acid cycle. As a precursor of amino acids such as glutamine and glutamic acid, α-KG plays a direct role in energy production and a wide range of cellular chemical reactions. α-KG provides an energy source, stimulating protein synthesis, inhibiting protein degradation in muscle, and serving as a significant metabolic fuel for gastrointestinal cells.
α-KG promotes osteogenic differentiation of stem cells, increases activity of osteoblasts to promote osteogenesis, and inhibits bone resorption activity of osteoclasts. α-KG in articular cartilage promotes differentiation and maturation of chondrocytes and formation of a cartilage matrix. The protective effect of α-KG on bone has practical value in treatment of abnormal bone loss symptoms in various bone tissue diseases.”
A rodent study explored adding α-KG to osteoarthritis treatment:
“Mesenchymal stem cell (MSC) therapy represents a promising treatment strategy for osteoarthritis (OA). Nevertheless, the therapeutic efficacy of MSCs may be attenuated under conditions of cellular senescence or when the available clinical quantity is insufficient. α-Ketoglutarate (AKG) exerts beneficial effects on skeletal tissues and activity of stem cells. The present study was designed to explore the potential of AKG in augmenting viability of MSCs and the potential of their combined utilization in treatment of OA.
AKG plays a crucial role in multiple biological processes. It is involved in regulating stem cell differentiation, exerts anti-apoptotic effects, modulates the body’s immune and inflammatory responses, contributes to muscle and bone development, and is essential for maintaining stability of the cartilage matrix.
Platelet-rich plasma (PRP) has been demonstrated to have protective effects on chondrocytes and can effectively repair damaged cartilage in OA. However, PRP has intractable problems in terms of product quality control and allogeneic application, and its long-term therapeutic effect gradually weakens.
Combining AKG’s regulation of cellular metabolism with the multi-directional differentiation and immunomodulatory functions of MSCs is likely to generate a synergistic effect. This combined treatment modality targets the complex pathological processes of OA, including cartilage damage, inflammatory responses, and extracellular matrix imbalance, in a more comprehensive manner than a single therapy.”
A rodent study investigated whether α-KG has a role in determining frailty:
“Frailty is an age-related geriatric syndrome, for which the mechanisms remain largely unknown. We performed a longitudinal study of aging female (n = 40) and male (n = 47) C57BL/6NIA mice, measured frailty index, and derived metabolomics data from plasma samples.
We find that frailty related metabolites are enriched for amino acid metabolism and metabolism of cofactors and vitamins, include ergothioneine, tryptophan, and alpha-ketoglutarate, and present sex dimorphism. We identify B vitamin metabolism related flavin adenine dinucleotide and pyridoxate as female-specific frailty biomarkers, and lipid metabolism related sphingomyelins, glycerophosphoethanolamine and glycerophosphocholine as male-specific frailty biomarkers.
We were interested to observe whether metabolite abundance at any specific timepoint was associated with frailty at a future timepoint. Unfortunately, we didn’t observe any metabolites that showed an overall significant association with future FI (FIf) or future devFI (devFIf). When focusing only on the abundance of metabolites at the baseline time point (∼400 days), we found a single metabolite, alpha-ketoglutarate, was negatively associated with both FIf and devFIf.”
Wrapping up with a rodent study adding α-KG to exercise for its effects on depression and learning:
“aKG acts as a prophylactic and antidepressant to effectively counteract social avoidance behaviors by modulating BDNF levels in the hippocampus and nucleus accumbens. Exercise increases aKG levels in the circulation.
In mice, aKG supplementation prolongs lifespan and reduces aging-associated frailty. aKG supplementation also reverses aging in humans as measured by DNA methylation patterns.
aKG functions as a co-factor for epigenetic enzymes. Changes in the intracellular αKG/succinate ratio regulates chromatin modifications, including H3K27me3 and ten-eleven translocation (Tet)-dependent DNA demethylation. The ability of aKG to influence epigenetic status of cells may explain both its prophylactic and anti-depressant effects since transcriptional dysregulation and aberrant epigenetic regulation are unifying themes in psychiatric disorders. This may also explain its ability to differentially regulate BDNF expression in the hippocampus and NAc.
If exercise mediates its effects through aKG, aKG may be a pivotal component of an exercise pill along with lactate and BHB that can serve as both a prophylactic and antidepressant treatment for depression.”
This blog’s 1100th curation is a clinical trial of ergothioneine’s effects on cognitive decline:
“We recruited participants aged between 60–90 years of age, from three study cohorts diagnosed with mild cognitive impairment (MCI) and provided them with ergothioneine (ET) (25 mg capsules administered orally three times a week) or placebo in a double-blinded and randomized manner. Blood samples were collected at baseline and quarterly (visits 1, 4, 7, 10, 14) for clinical safety assessment and biomarker analyses). Neuro-cognitive assessments were conducted biannually (visits 7 and 14).
Following ET intake, an increase in Z-scores was observed in the Rey Auditory Verbal Learning Test (RAVLT) (immediate and delayed recalls), which evaluates learning ability and memory.
Participants in both ET and placebo groups recorded a lower total white blood cell count compared to baseline at visit 7, both of which recovered subsequently. The reasons for this anomaly are unclear but values were all still within the expected range for their age.”
I rated this study a waste of time and money for the researchers’ incurious lack of following where their data led. Significant WBC signals of both treatment and placebo subjects’ immune system responses were shrugged off with an “expected range” non-explanation.
Two 2024 reviews by the same group that published Sulforaphane in the Goldilocks zone investigated dietary polyphenols’ effects as “hormetic nutrients”:
“Polyphenols display biphasic dose–response effects by activating at a low dose the Nrf2 pathway resulting in the upregulation of antioxidant vitagenes [see diagram]. We aimed to discuss hormetic nutrients, including polyphenols and/or probiotics, targeting the Nrf2 pathway and vitagenes for the development of promising neuroprotective and therapeutic strategies to suppress oxidative stress, inflammation and microbiota deregulation, and consequently improve cognitive performance and brain health.
Hormetic nutrition through polyphenols and/or probiotics targeting the antioxidant Nrf2 pathway and stress resilient vitagenes to inhibit oxidative stress and inflammatory pathways, as well as ferroptosis, could represent an effective therapy to manipulate alterations in the gut microbiome leading to brain dysfunction in order to prevent or slow the onset of major cognitive disorders. Notably, hormetic nutrients can stimulate the vagus nerve as a means of directly modulating microbiota-brain interactions for therapeutic purposes to mitigate or reverse the pathophysiological process, restoring gut and brain homeostasis, as reported by extensive preclinical and clinical studies.”
I’m not onboard with this study’s probiotic assertions because most of the cited studies contained unacknowledged measurement errors. Measuring gut microbiota, Part 2 found:
“The fecal microbiome does not represent the overall composition of the gut microbiome. Despite significant roles of gut microbiome in various phenotypes and diseases of its host, causative microbes for such characteristics identified by one research fail to be reproduced in others.
Since fecal microbiome is a result of the gut microbiome rather than the representative microbiome of the GI tract of the host, there is a limitation in identifying causative intestinal microbes related to these phenotypes and diseases by studying fecal microbiome.”
These researchers also erroneously equated isothiocyanate sulforaphane’s Nrf2-activating mechanisms with polyphenols activating Nrf2.
This research group did better in clarifying polyphenols’ mechanisms in a review of hormetic dose-response effects of the polyphenol rosmarinic acid:
“This article evaluates whether rosmarinic acid may act as a hormetic agent, mediating its chemoprotective effects as has been shown for similar agents, such as caffeic acid, a derivative of rosmarinic acid.
Rosmarinic acid enhanced memory in institute of cancer research male mice in the Morris water maze (escape latency).
Of importance in the evaluation of rosmarinic acid are its bioavailability, metabolism, and tissue distribution (including the capacity to affect and/or cross the BBB and its distribution and half-life within the brain). In the case of polyphenols, including rosmarinic acid, they are typically delivered at low doses in the diet and, in most instances, they do not escape first-pass metabolism, with the prominent chemical forms being conjugates of glucuronides and sulfates, with or without methylation.
These conjugated metabolites are chemically distinct from the parent compound, showing considerable differences in size, polarity, and ionic form. Their biological actions are quite different from the parent compound.
Bioavailability studies reveal that maximum concentrations in plasma typically do not exceed 1 µM following consumption of 10–100 mg of a single phenolic compound, with the maximum concentration occurring typically less than 2 h after ingestion, then dropping quickly thereafter. In the case of the in vitro studies assessed herein, and with few exceptions, most of the studies employed concentrations >10 µM with some studies involving concentrations in the several hundred µM range, with the duration of exposure typically in the range of 24–72 h, far longer duration than the very short time interval of a few minutes to several hours in human in vivo situations.
We strongly recommend that all experiments using in vitro models to study biological responses to dietary polyphenols use only physiologically relevant flavonoids and their conjugates at appropriate concentrations, provide evidence to support their use, and justify any conclusions generated. When authors fail to do this, referees and editors must act to ensure that data obtained in vitro are relevant to what might occur in vivo.”
An excerpt from the latest video at Dr. Goodenowe’s Health Matters podcast, Episode 7 “The Truth about Parkinson’s”, starting at 50:30:
“What’s exciting about this community medicine focus that we’ve switched to which basically says: How do we develop technologies in a way that they can be incorporated into a community model versus a pharmaceutical drug model? People can actually do I would say self-experiment just the way you self-experiment with your own diet because these are fundamentally dietary nutrition molecules.
Could you give me an elevator pitch because there are probably people listening who are thinking what is this plasmalogen precursor and for sure how is it having this dramatic effect?
Plasmalogens are the most important nutrient that nobody knows about. Normally you don’t know about it because the body is usually pretty good at making them. What makes plasmalogens unique is that your body makes them kind of like cannon fodder, the first group of people that go into war. Your body throws them out for destruction. They absorb oxidative stress and get destroyed in the process.
They’re stored in your cell membranes. 50% of the membranes of your heart are these plasmalogen molecules. When your heart gets inflamed, what your heart does is it dumps these plasmalogens out of its membranes to douse the flame of inflammation. After inflammation is under control, your body naturally builds these things back up again.
But if you have an inability to make enough plasmalogens, these inflammation events knock you down and keep you down. So plasmalogen precursors are critical for maintaining high levels of plasmalogens across your body, not just in your brain (30% of the lipids in your brain) but in your heart, your lungs, your kidneys.”