Two sulforaphane topics came up in discussions with my traveling companion. Our first was an inference:
- 3-day-old broccoli sprouts have the optimal yields found that broccoli sprout sulforaphane content (after processing for analysis) ranged from 46% to 97% of broccoli seeds.
- Microwave broccoli to increase sulforaphane levels found that microwaving broccoli florets to 60°C (140°F) increased the sulforaphane amount from .22 to 2.45 µmol / g (1,114%!!).
- Wouldn’t broccoli seeds’ sulforaphane be more than broccoli sprouts by microwaving seeds up to 60°C in the same amount of water?
The 3-day study broccoli sprout measurements were relative to each variety’s seeds:
“To be comparable, the content of these bioactive compounds from 100 fresh sprouts was divided by the weight (gram) of 100 seeds, and then this value was compared with their content from one gram seeds.”
Broccoli compounds are similar among broccoli florets, sprouts, and seeds. A major difference is that broccoli sprouts and seeds have no initial sulforaphane content because hydrolization hasn’t occurred yet. The above graphic’s seed and sprout sulforaphane content was created by processing for analysis.
I’ll reason that sulforaphane would be created by:
- Microwaving one tablespoon of broccoli seeds with a 1000W microwave in 100 ml of distilled water for 30 seconds to ≤ 60°C; then
- Straining out the water; then
- Allowing further myrosinase hydrolization of glucoraphanin and other glucosinolates into sulforaphane and other healthy compounds.
Broccoli seeds are dry, and microwaving acts directly on a material’s water content. The 3-day study methods “immersed [broccoli seeds] in distilled water and soaked at 30°C for 2 h” to start germination. I’ll stipulate two hours as a minimum broccoli seed soaking time before microwaving.
I’ve tried microwaving broccoli seeds five times so far to see if they’re palatable. Seeds soaked for at least two hours then microwaved for 30 seconds swell to almost twice their dry size. They’re easier to strain, chew thoroughly to ensure hydrolization, and swallow.
The 3-day study also found “total phenolic and flavonoid contents in sprouts were 1.12 to 3.58 times higher than seeds.” I won’t stop eating broccoli sprouts, but sometimes it may be expedient to reduce a 72-hour preparation time to 2 hours and still benefit from sulforaphane and other healthy broccoli compounds.
Let’s use Estimating daily consumption of broccoli sprout compounds runt-of-the-litter calculations and assumptions to make a worst-case estimate of sulforaphane content in one tablespoon of broccoli seeds:
- Broccoli seed weight of one tablespoon
- Worst-case sulforaphane weight in one tablespoon of broccoli seeds (10.7 g x 2.43 mg sulforaphane per gram of seeds) = 26.0 mg.
I won’t calculate
“Broccoli seeds were comminuted by analysis grinder. Seed powder (0.5g) was immersed in distilled water at 55 °C for 5 min to inactivate the epithiospecifier protein.”
Grinding seeds into powder then heating it probably incorporates any effects of microwaving intact broccoli seeds up to 60°C.
Our second discussion topic came by gathering study data from Broccoli or Sulforaphane: Is It the Source or Dose That Matters?

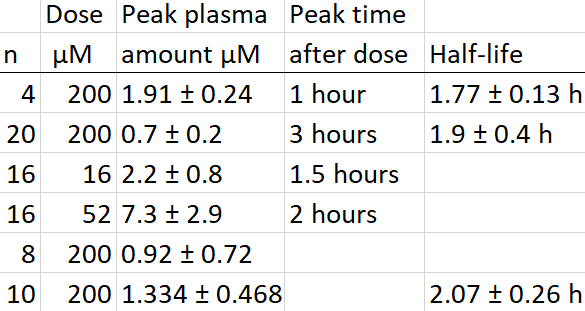
Assessing these 200 μmol amount / 35 mg weight sulforaphane supplement dose studies:
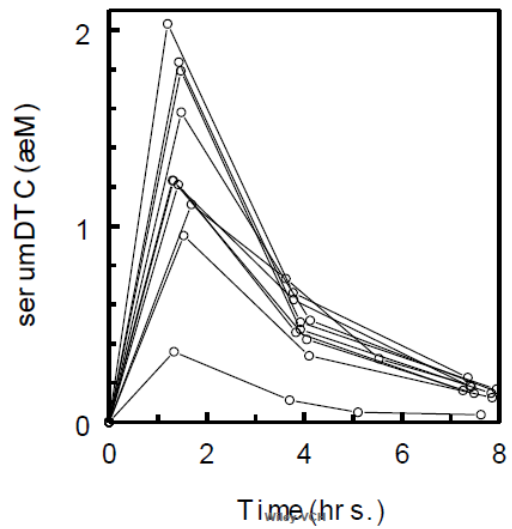
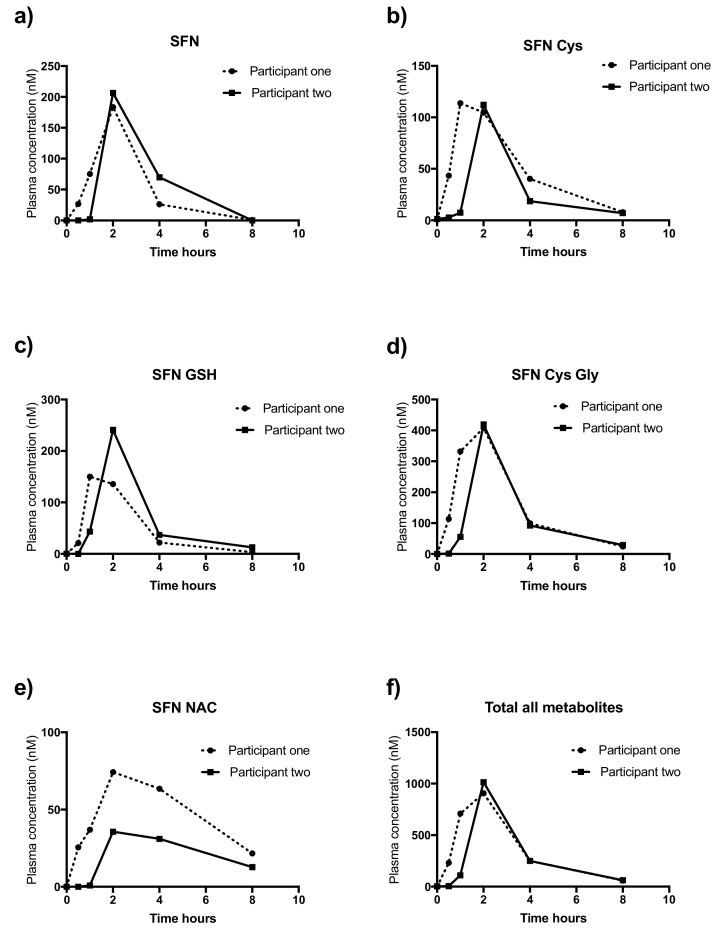
- Peak plasma statistics ranged from 0.5 μmol in Row 2 (n = 20) to 2.15 (n = 4) μmol in Row 1. Row 4 (n = 10) statistics don’t show it, but its individual peak plasma ranges per the below graphic were 0.359 μmol to 2.032 μmol. Coincidentally, the Row 4 subject (#2) who had the lowest peak plasma amount also had the lowest urinary % of dose excreted (also termed bioavailability) of 19.5%, and the Row 4 subject (#8) who had the highest peak plasma amount also had the highest sulforaphane bioavailability of 86.9%.

- From the Row 4 study: “The half-life of SF in the body was 2.07 ± 0.26 h as calculated from serum area-under-the-curve determinations.” Its Subject #2 had the longest sulforaphane half-life at 2.709 hours.
- The peak time after dose ranged from 1 to 3 hours. Not sure why Row 4 didn’t calculate a peak time, but eyeballing the above graphic showed that all subjects peaked between 1 and 2 hours. Row 2’s time was at the study’s first of three measurement intervals (3, 6, and 12 hours). Its peak time after dose probably also took place between 1 and 2 hours.
These four studies showed that there’s wide variation among individual responses to sulforaphane supplements. Row 4 study’s Concluding Remarks ended with:
“Innate metabolic differences must not be discounted when assessing the metabolism of SF alone, delivered in supplements.”
The first of A pair of broccoli sprout studies was Row 2 (n = 20) above. Its sulforaphane supplement statistics – repeated in the below graphic’s BSE (broccoli sprout extract) column – demonstrated how humans’ sulforaphane supplement metabolic profiles were different than our fresh broccoli sprout metabolic profiles:

The divided dose was twelve hours apart at breakfast and dinner times. Also, its first measurements weren’t taken until 3 hours after ingesting, which explains its later times with lesser amounts than the above sulforaphane supplement studies’ earlier times with greater amounts.
During Week 9 of Changing to a youthful phenotype with broccoli sprouts I changed my practices to eat microwaved broccoli sprouts at breakfast and dinner times from its finding:
“In sprout consumers, plasma concentrations were 2.4-fold higher after consuming the second dose than after the first dose.”
A metabolic profile resulting from my current practices is probably between the Sprout and BSE divided-dose statistics:
- Sulforaphane intake is greater than eating raw broccoli sprouts because microwaving 3-day-old broccoli sprouts creates sulforaphane in them before eating.
- Sulforaphane uptake from microwaved broccoli sprouts is quicker than eating raw broccoli sprouts. It may not be as immediate as taking sulforaphane supplements, which are usually powders.
- Sulforaphane dose from microwaved broccoli sprouts is less dependent on an individual’s metabolism than eating raw broccoli sprouts.
- Sulforaphane release from microwaved broccoli sprouts probably continues on to the gut as does eating raw broccoli sprouts. Sulforaphane release from supplements may not per Does sulforaphane reach the colon?.
The microwaving study processed 10 grams of broccoli florets immersed in 500 ml water with a 950W microwave on full power for 108 seconds to achieve 60°C. I microwave
After microwaving I wait five minutes to allow further myrosinase hydrolization of glucoraphanin and other glucosinolates into sulforaphane and other healthy compounds. Enhancing sulforaphane content provided evidence that myrosinase hydrolization peaks at one minute after achieving 60°C per the below graphic:
I interpret the above sulforaphane degradation from minutes 1 to 5 to be leaching caused by leaving the broccoli sample immersed in water. I strain water from broccoli sprouts after microwaving – the Time 0 mark of the above graphic – because without leaching water, further hydrolization may increase sulforaphane.
Sulforaphane supplements:
- Are readily metabolized,
- Blood plasma levels peak by two hours, and
- Blood plasma levels dissipate by eight hours.
To the extent a metabolism resulting from my current practices is closer to a sulforaphane supplement profile than a raw broccoli sprouts profile, maybe that leaves the door open to a microwaved broccoli seed dose at lunch time? In any event, there are seeds in each batch that don’t germinate after soaking for 12 hours and rinsing three times a day, and I eat them after microwaving anyway.
See Caution on broccoli seed erucic acid content? if you’re concerned about that.















 Living beings – thousands of years old – living together
Living beings – thousands of years old – living together