People will forgive you for being wrong, but they will never forgive you for being right – especially if events prove you right while proving them wrong. Thomas Sowell
This 2019 Spanish human study used improved techniques to find:
“Adult hippocampal neurogenesis (AHN), confers an unparalleled degree of plasticity to the entire hippocampal circuitry. Direct evidence of AHN in humans has remained elusive. Determining whether new neurons are continuously incorporated into the human dentate gyrus (DG) during physiological and pathological aging is a crucial question with outstanding therapeutic potential.
By combining human brain samples obtained under tightly controlled conditions and state-of-the-art tissue processing methods, we identified thousands of immature neurons in the DG of neurologically healthy human subjects up to the ninth decade of life. These neurons exhibited variable degrees of maturation along differentiation stages of AHN. In sharp contrast, the number and maturation of these neurons progressively declined as AD advanced.
These results demonstrate the persistence of AHN during both physiological and pathological aging in humans and provide evidence for impaired neurogenesis as a potentially relevant mechanism underlying memory deficits in AD that might be amenable to novel therapeutic strategies.”
The control group was 13 neurologically healthy deceased people aged 43 to 87. The AD group was 45 deceased people, distributed among the six Braak stages of the pathology, aged 52 to 97.
This 2019 Spanish human study compared DNA methylation, chromatin and histone modifications in the hippocampus of deceased Alzheimer’s disease patients with controls:
“A significant percentage of the differentially methylated genes were related to neural development and neurogenesis. It was astounding that other biological, cellular, and molecular processes generally associated with neurodegeneration such as apoptosis, autophagy, inflammation, oxidative stress, and mitochondrial or lysosomal dysfunction were not overrepresented.
The results of the present study point to neurogenesis-related genes as targets of epigenetic changes in the hippocampus affected by AD. These methylation changes might be built throughout life due to external and internal cues and would represent an example of epigenetic interaction between environmental and genetic factors in developing AD.
As an alternative explanation, these epigenetic marks might also represent the trace of DNA methylation alterations induced during early developmental stages of the hippocampus, which would remain as a fingerprint in the larger proportion of hippocampal neurons that are not exchanged. This second hypothesis would link AD to early life stages, in concordance with recent studies that revealed abnormal p-tau deposits (pre-tangles) in brains of young individuals under 30, suggesting AD pathology would start earlier in life than it was previously thought. The influence of the genetic risk for AD has also been postulated to begin in early life, and other AD risk factors may be influenced by in utero environment.”
The study cited references to adult neurogenesis:
“Though strongly related to brain development, neurogenesis is also maintained in the adult human brain, mainly in two distinct areas, i.e., the subventricular zone and the subgranular zone of the dentate gyrus in the hippocampus. There is substantial neurogenesis throughout life in the human hippocampus as it is estimated that up to one third of human hippocampal neurons are subject to constant turnover.
Adult neurogenesis is linked to hippocampal-dependent learning and memory tasks and is reduced during aging. Recent evidence suggests that adult neurogenesis is altered in the neurodegenerative process of AD, but it is still controversial with some authors reporting increased neurogenesis, whereas others show reduced neurogenesis. In the human hippocampus, a sharp drop in adult neurogenesis has been observed in subjects with AD.”
One of the study’s limitations was its control group:
“There was a significant difference in age between controls [12, ages 50.7 ± 21.5] and AD patients [26, ages 81.2 ± 12.1], being the latter group older than the former group. Although we adjusted for age in the statistical differential methylation analysis, the accuracy of this correction may be limited as there is little overlap in the age ranges of both groups.”
This 2019 New York rodent study investigated multiple avenues to uncover mechanisms of obsessive-compulsive disorder:
“Psychophysical models of OCD propose that anxiety (amygdala) and habits (dorsolateral striatum) may be causally linked. Numerous genetic and environmental factors may reduce striatum sensitivity and lead to maladaptive overcompensation, potentially accounting for a significant proportion of cases of pathological OCD-like behaviors.
Our results indicate that both the development and reversal of OCD-like behaviors involve neuroplasticity resulting in circuitry changes in BLA-DLS and possibly elsewhere.”
The researchers explored two genetic models of OCD, showed why these insufficiently explained observed phenomena, then followed up with epigenetic investigations. They demonstrated how and the degree to which histone modifications and DNA methylation regulated both the development and reversal of OCD symptoms.
However, the researchers also carelessly cited thirteen papers outside the specific areas of the study to support one statement in the lead paragraph:
“Novel studies propose that modulations in gene expression influenced by environmental factors, are connected to mental health disorders.”
Only one of the thirteen citations was more recent than 2011, and none of them were high-quality studies.
This 2019 UK review discussed delusions, aka false beliefs about reality:
“Delusions are characterized by their behavioral manifestations and defined as irrational beliefs that compromise good functioning. In this overview paper, we ask whether delusions can be adaptive notwithstanding their negative features.
We consider different types of delusions and different ways in which they can be considered as adaptive: psychologically (e.g., by increasing wellbeing, purpose in life, intrapsychic coherence, or good functioning) and biologically (e.g., by enhancing genetic fitness).”
A. Although section 4’s heading was Biological Adaptiveness of Delusions, the reviewers never got around to discussing evolved roles of brain areas and beliefs (delusions). One mention of evolutionary biology was:
“Delusions are biologically adaptive if, as a response to a crisis of some sort (anomalous perception or overwhelming distress), they enhance a person’s chances of reproductive success and survival by conferring systematic biological benefits.”
B. Although section 5’s heading was Psychological Adaptiveness of Delusions, the reviewers didn’t connect feelings and survival sensations as origins of beliefs (delusions) and behaviors. They had a few examples of feelings:
“Delusions of reference and delusions of grandeur can make the person feel important and worthy of admiration.”
and occasionally sniffed a clue:
“Some delusions (especially so‐called motivated delusions) play a defensive function, representing the world as the person would like it to be.”
where “motivated delusions” were later deemed in the Conclusion section to be a:
“Response to negative emotions that could otherwise become overwhelming.”
C. Feelings weren’t extensively discussed until section 6 Delusions in OCD and MDD, which gave readers an impression that feelings were best associated with those diseases.
D. In the Introduction, sections 4, 5, and 7 How Do We Establish and Measure Adaptiveness, the reviewers discussed feeling meaning in life, but without understanding:
“Without feeling, life becomes empty and sterile. It, above all, loses its meaning.“
Beliefs (delusions) defend against feelings.
Consequentially, the stronger and / or more numerous beliefs (delusions) a person has, the less they feel meaning in life.
E. Where, when, why, and how do beliefs (delusions) arise? Where, when, why, and how does a person sense and feel, and what are the connections with beliefs (delusions)?
F. The word “sense” was used 29 times in contexts such as “make sense” and “sense of [anxiety, coherence, control, meaning, purpose, rational agency, reality, self, uncertainty]” but no framework connected biological sensing to delusions. Papers from other fields have detailed cause-and-effect explanations and predecessor-successor diagrams for every step of a process. Not this one.
Regarding any therapeutic value of someone else’s opinion of a patient’s delusions:
I’ll reuse this quotation from the Scientific evidence page of Dr. Janov’s 2011 book “Life Before Birth: The Hidden Script that Rules Our Lives” p.166:
“Primal Therapy differs from other forms of treatment in that the patient is himself a therapist of sorts. Equipped with the insights of his history, he learns how to access himself and how to feel.
The therapist does not heal him; the therapist is only the catalyst allowing the healing forces to take place. The patient has the power to heal himself.“
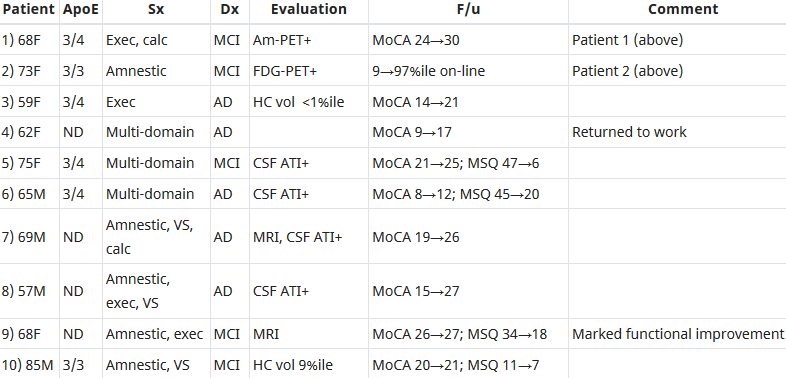
This 2018 human study presented the results of 100 patients’ personalized therapies for cognitive decline:
“The first examples of reversal of cognitive decline in Alzheimer’s disease and the pre-Alzheimer’s disease conditions MCI (Mild Cognitive Impairment) and SCI (Subjective Cognitive Impairment) have recently been published..showing sustained subjective and objective improvement in cognition, using a comprehensive, precision medicine approach that involves determining the potential contributors to the cognitive decline (e.g., activation of the innate immune system by pathogens or intestinal permeability, reduction in trophic or hormonal support, specific toxin exposure, or other contributors), using a computer-based algorithm to determine subtype and then addressing each contributor using a personalized, targeted, multi-factorial approach dubbed ReCODE for reversal of cognitive decline.
An obvious criticism of the initial studies is the small number of patients reported. Therefore, we report here 100 patients, treated by several different physicians, with documented improvement in cognition, in some cases with documentation of improvement in electrophysiology or imaging, as well.”
“We have a paper in press, due to appear 10.22.18 (open access, JADP, I’ll send a copy as soon as available), showing 100 patients with documented improvement – some with MRI volumetrics improved, others with quantitative EEG improvements, others with evoked response improvements, and all with quantitative cognitive assessment improvement. Some are very striking – 12 point improvements in MoCA [Montreal Cognitive Assessment], for example – others less so, but all also have subjective improvement. Hopefully this will address some of the criticisms that we haven’t documented improvement in enough people.
We were just turned down again for a randomized, controlled clinical trial, so on the one hand, we are told repeatedly that no one will believe that this approach works until we publish a randomized, controlled study, and on the other hand, we’ve been turned down (first in 2011/12, and now in 2018), with the complaint that we are trying to address more than one variable in the trial (as if AD is a single-variable disease!). Something of a catch-22. We are now resubmitting (unfortunately, the IRBs are not populated by functional medicine physicians, so they are used to seeing old-fashioned drug studies), and we’ll see what happens.
I’ve been extending the studies to other neurodegenerative diseases, and it has been impressive how much of a programmatic response there seems to be in these ‘diseases.’
I agree with you that there are many features in common with aging itself.
You made a good point that APP [amyloid precursor protein] is a dependence receptor, and in fact it functions as an integrating dependence receptor, responding to numerous inputs (Kurakin and Bredesen, 2015).
In the book and the publications, we don’t claim it is a “cure” since we don’t have pathological evidence that the disease process is gone. What we claim is ‘reversal of cognitive decline’ since that is what we document.
As I mentioned in the book, AD is turning out to be a protective response to multiple insults, and this fits well with the finding that Abeta has an antimicrobial effect (Moir and Tanzi’s work). It is a network-downsizing, protective response, which is quite effective – some people live with the ongoing degenerative process for decades.
We have seen several cases now in which a clinical trial of an anti-amyloid antibody made the person much worse in a time-dependent manner (each time there was an injection, the person would get much worse for 5-10 days, then begin to improve back toward where he/she was, but over time, marked decline occurred), and this makes sense for the idea that the amyloid is actually protecting against pathogens or toxins or some other insult.
It is important to note that we’ve never claimed that all people get better – this is not what we’ve seen. People very late in the process, or who don’t follow the protocol, or who don’t address the various insults, do not improve. It is also turning out to be practitioner dependent – some are getting the vast majority of people to improve, others very few, so this is more like surgery than old-fashioned prescriptive medicine – you have to do a somewhat complicated therapeutic algorithm and get it right for best results.
I’m very interested in what is needed to take the next step in people who have shown improvement but who started late in the course. For example, we have people now who have increased MoCA from 0 to 9 (or 0 to 3, etc.), with marked subjective improvement but plateauing at less than normal. These people had extensive synaptic and cellular loss prior to the program. So what do we need to raise the plateau? Stem cells? Intranasal trophic support? Something else?
I haven’t yet seen a mono-etiologic theory of AD or a mono-therapeutic approach that has repeatedly positive results, so although I understand that there are many theories and treatments, there doesn’t seem to be one etiology to the disease, nor does there seem to be one simple treatment that works for most. It is much more like a network failure.”
At a specific level:
“There doesn’t seem to be one etiology to the disease,
Nor does there seem to be one simple treatment that works for most.
We don’t have pathological evidence that the disease process is gone.”
For general concepts, however:
“AD is turning out to be a protective response to multiple insults.
It is a network-downsizing, protective response, which is quite effective.
The amyloid is actually protecting against pathogens or toxins or some other insult.”
For a framework of an AD cure to be valid, each source of each insult that evoked each “protective response” should be traced.
Longitudinal studies would be preferred inside this framework. These study designs would investigate evidence of each insult’s potential modifying effect on each “protective response” that could affect the cumulative disease trajectory of each individual.
In many cases, existing study designs would be adequate if they extended their periods to the end of the subjects’ natural lifetimes. One AD-relevant example would be extending the prenatally-restraint-stressed model used in:
The framework would also encourage extending studies to at least three generations to investigate evidence for transgenerational effects, as were found in:
“For half a century, a high level of total cholesterol (TC) or low-density lipoprotein cholesterol (LDL-C) has been considered to be the major cause of atherosclerosis and cardiovascular disease (CVD), and statin treatment has been widely promoted for cardiovascular prevention. However, there is an increasing understanding that the mechanisms are more complicated and that statin treatment, in particular when used as primary prevention, is of doubtful benefit.
The authors of three large reviews recently published by statin advocates have attempted to validate the current dogma. This article delineates the serious errors in these three reviews as well as other obvious falsifications of the cholesterol hypothesis.
Our search for falsifications of the cholesterol hypothesis confirms that it is unable to satisfy any of the Bradford Hill criteria for causality and that the conclusions of the authors of the three reviews are based on:
Misleading statistics,
Exclusion of unsuccessful trials and by
Ignoring numerous contradictory observations.
The association between the absolute risk reduction of total mortality in 26 statin trials [squares] included in the study by Silverman et al. and in 11 ignored trials [triangles] and the year where the trial protocols were published. The vertical line indicates the year where the new trial regulations were introduced.
In 2004–2005, health authorities in Europe and the United States introduced New Clinical Trial Regulations, which specified that all trial data had to be made public. Since 2005, claims of benefit from statin trials have virtually disappeared.”
This paradigm was proven wrong eighty years ago! How much longer will its harmful consequences continue?
Starting the fifth year of this blog with a 2018 presentation by the founder of the epigenetic clock method describing the state of the art up through July 2018. The webinar was given on the release day of The epigenetic clock now includes skin study.
Segments before the half-hour mark provide an introduction to the method and several details about the concurrently-released study. The Q&A section starts a little before the hour mark.
This 2018 Chinese animal review subject was prenatal and perinatal anesthesia’s adverse epigenetic effects on a fetus/neonate:
“Accumulating evidence from rodent and primate studies has demonstrated that in utero or neonatal exposure to commonly used inhaled and intravenous general anesthetics is associated with neural degeneration and subsequent neurocognitive impairments, manifested in learning and memory disabilities.
So far, conflicting data exist about the effect of anesthetic agents on neurodevelopment in humans and no definite conclusion has been given yet.”
The inhibitors in the above graphic counter anesthesia’s effects on the fetus/neonate, summarized as:
“Epigenetic targeting of DNA methyltransferases and/or histone deacetylases may have some therapeutic value.”
Do physicians consider possible epigenetic alterations of a newborn’s chromatin structure and gene expression when they administer anesthesia to mothers during childbirth?
This 2018 Chinese review highlighted areas in which CRISPR/Cas9 technology has, is, and could be applied to rewrite epigenetic changes:
“CRISPR/Cas9-mediated epigenome editing holds a great promise for epigenetic studies and therapeutics.
It could be used to selectively modify epigenetic marks at a given locus to explore mechanisms of how targeted epigenetic alterations would affect transcription regulation and cause subsequent phenotype changes. For example, inducing histone methylation or acetylation at the Fosb locus in the mice brain reward region, nucleus accumbens, could affect relevant transcription network and thus control behavioralresponses evoked by drug and stress.
Epigenome editing has the potential for epigenetic treatment, especially for the disorders with abnormal gene imprinting or epigenetic marks. Targeted epigenetic silencing or reactivation of the mutant allele could be a potential therapeutic approach for diseases such as Rett syndrome and Huntington’s disease.
Noncoding RNA plays important roles in gene imprinting and chromatin remodeling. CRISPR/Cas9 has been shown to be potential for manipulating noncoding RNA expression, including microRNA, long noncoding RNA, and miRNA families and clusters.
In vivo overexpression of the Yamanaka factors have proven to be able to fully or partially help somatic cells to regain pluripotency in situ. These rejuvenated cells would subsequently differentiate again to replace the lost cell types.”
“To date, the most effective in vitro intervention against epigenetic ageing is achieved through expression of Yamanaka factors, which convert somatic cells into pluripotent stem cells, thereby completely resetting the epigenetic clock.”
The reviewers cited three references for in vivo studies of this technique. Overall, I didn’t see that any of the review’s references were in vivo human studies.
The originator of the 2013 epigenetic clock improved its coverage with this 2018 UCLA human study:
“We present a new DNA methylation-based biomarker (based on 391 CpGs) that was developed to accurately measure the age of human fibroblasts, keratinocytes, buccal cells, endothelial cells, skin and blood samples. We also observe strong age correlations in sorted neurons, glia, brain, liver, and bone samples.
The skin & blood clock outperforms widely used existing biomarkers when it comes to accurately measuring the age of an individual based on DNA extracted from skin, dermis, epidermis, blood, saliva, buccal swabs, and endothelial cells. Thus, the biomarker can also be used for forensic and biomedical applications involving human specimens.
The biomarker applies to the entire age span starting from newborns, e.g. DNAm of cord blood samples correlates with gestational week.
Furthermore, the skin & blood clock confirms the effect of lifestyle and demographic variables on epigenetic aging. Essentially it highlights a significant trend of accelerated epigenetic aging with sub-clinical indicators of poor health.
Conversely, reduced aging rate is correlated with known health-improving features such as physical exercise, fish consumption, high carotenoid levels. As with the other age predictors, the skin & blood clock is also able to predict time to death.
Collectively, these features show that while the skin & blood clock is clearly superior in its performance on skin cells, it crucially retained all the other features that are common to other existing age estimators.”
An introduction to the study highlighted several items:
“Although the skin-blood clock was derived from significantly less samples (~900) than Horvath’s clock (~8000 samples), it was found to more accurately predict chronological age, not only across fibroblasts and skin, but also across blood, buccal and saliva tissue. A potential factor driving this improved accuracy in blood could be related to the approximate 18-fold increase in genomic coverage afforded by using Illumina 450k/850k beadarrays.
It serves as a roadmap for future clock studies, pointing towards the importance of constructing tissue or cell-type specific epigenetic clocks, to more accurately measure biological aging in the given tissue/cell-type, and therefore with the potential to be more informative of disease-risk or the success of disease interventions in the tissue or cell-type of interest.”
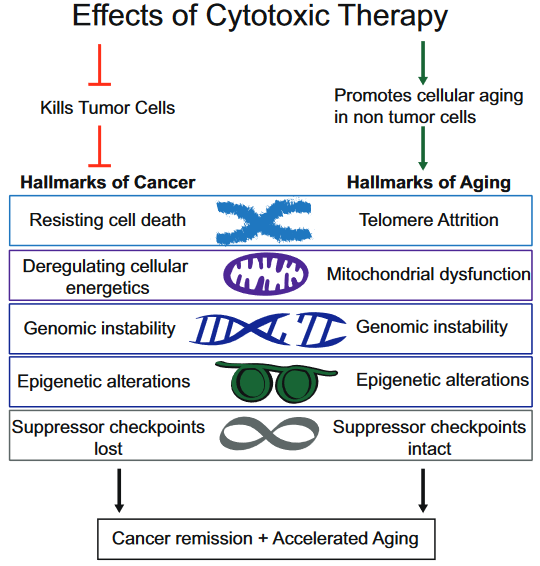
This 2018 UC San Diego review subject was the interplay between breast cancer treatments and their effects on aging:
“Although current breast cancer treatments are largely successful in producing cancer remission and extending lifespan, there is concern that these treatments may have long lasting detrimental effects on cancer survivors, in part, through their impact on non-tumor cells. It is unclear whether breast cancer and/or its treatments are associated with an accelerated aging phenotype.
In this review, we have highlighted five of nine previously described cellular hallmarks of aging that have been described in the context of cytotoxic breast cancer treatments:
The review was full of caveats weakening the above graphic’s associations:
“Telomere attrition – Blood TL [telomere length] was not associated with chemotherapy in three out of four studies;
Mitochondrial dysfunction – How cancer therapies affect cellular energetics as they relate to rate of aging is unclear;
Genomic instability – Potentially contributing to accelerated aging;
Epigenetic alterations – Although some of the key regulators of these processes have begun to be identified, including DNA and histone methylases and demethylases, histone acetylases and de-acetylases and chromatin remodelers, how they regulate the changes in aging through alteration of global transcriptional programs, remains to be elucidated; and
Cellular senescence – Dysregulated pathways can be targeted by cytotoxic chemotherapies, resulting in preferential cell death of tumor cells, but how these treatments also affect normal cells with intact pathways is unclear.”
To their credit, these reviewers at least presented some of the contrary evidence, and didn’t continue on with a directed narrative as other reviewers are prone to do.
The originator of the epigenetic clock methodology was a coauthor of the review. Only one of his works was cited in the Epigenetic alterations subsection:
This freely-available 2017 study quoted below highlighted that epigenetic clock measurements as originally designed were tissue-specific:
“To our knowledge, this is the first study to demonstrate that breast tissue epigenetic age exceeds that of blood tissue in healthy female donors. In addition to validating our earlier finding of age elevation in breast tissue, we further demonstrate that the magnitude of the difference between epigenetic age of breast and blood is highest in the youngest women in our study (age 20–30 years) and gradually diminishes with advancing age. As women approach the age of the menopausal transition, we found that the epigenetic of age of blood approaches that of the breast.”
Additional caution was justified in both interpreting age measurements and extending them into “cellular hallmarks” when the tissue contained varying cell types:
“Our studies were performed on whole breast tissue. Diverse types of cells make up whole breast tissue, with the majority of cells being adipocytes. Other types of cells include epithelial cells, cuboidal cells, myoepithelial cells, fibroblasts, inflammatory cells, vascular endothelial cells, preadipocytes, and adipose tissue macrophages.
This raises the possibility that the magnitude of the effects we observe, of breast tissue DNAm age being greater than other tissues, might be an underestimation, since it is possible that not all of the cells of the heterogenous sample have experienced this effect. Since it is difficult to extract DNA from adipose tissue, we suspect that the majority of DNA extracted from our whole breast tissues was from epithelial and myoepithelial cells.”
This 2018 Korean review discussed aspects of the hypothalamus and aging:
“A majority of physiological functions that decline with aging are broadly governed by the hypothalamus, a brain region controlling development, metabolism, reproduction, circadian rhythm, and homeostasis. In addition, the hypothalamus is poised to connect the brain and the body so that the environmental information affecting aging can be transmitted through the hypothalamus to affect the systematic aging of the peripheral organs.
The hypothalamus is hypothesized to be a primary regulator of the process of aging of the entire body. This review aims to assess the contribution of hypothalamic aging to the age-related decline in body functions, particularly from the perspective of:
energy homeostasis,
hormonal balance,
circadian rhythm, and
reproduction,
and to highlight its underlying cellular mechanisms with a focus on:
The reviewers didn’t consider aging to be an “unintended consequence” of development. This perspective was found in a reference to A study of DNA methylation and age:
“Aging is not programmed. Instead, aging is a continuation of developmental growth, driven by genetic pathways.
Genetic programs determine developmental growth and the onset of reproduction. When these programs are completed, they are not switched off.
Aging has no purpose (neither for individuals nor for group), no intention. Nature does not select for quasi-programs. It selects for robust developmental growth.”
“The proposed epigenetic clock theory of ageing views biological ageing as an unintended consequence of both developmental programmes and maintenance programmes.”
“The hypothalamus is hypothesized to be a primary regulator of the process of aging.”
Almost all of the details discussed were from rodent studies.
As detailed in How to cure the ultimate causes of migraines? and its references, the hypothalamus is a brain structure that lacks feedback mechanisms for several of its activities. This structure develops shortly after conception and has an active prenatal role.
The hypothalamus plays its part in getting us developed and ready to reproduce, with certain feedback loops being evolutionarily unnecessary. The hypothalamus perfectly illustrates the point of:
“When these programs are completed, they are not switched off.”
Evolutionarily unnecessary feedback for aspects of hypothalamic activity may result in it not winding down when its developmental role is over. This activity shouldn’t be interpreted to construe a role that has some other meaning or purpose.
This 2018 Loma Linda review subject was gestational hypoxia:
“Of all the stresses to which the fetus and newborn infant are subjected, perhaps the most important and clinically relevant is that of hypoxia. This review explores the impact of gestational hypoxia on maternal health and fetal development, and epigenetic mechanisms of developmental plasticity with emphasis on the uteroplacental circulation, heart development, cerebral circulation, pulmonary development, and the hypothalamic-pituitary-adrenal axis and adipose tissue.
An understanding of the specific hypoxia-induced environmental and epigenetic adaptations linked to specific organ systems will enhance the development of target-specific inhibition of DNA methylation, histone modifications, and noncoding RNAs that underlie hypoxia-induced phenotypicprogramming of disease vulnerability later in life.
A potential stumbling block to these efforts, however, relates to timing of the intervention. The greatest potential effect would be accomplished at the critical period in development for which the genomic plasticity is at its peak, thus ameliorating the influence of hypoxia or other stressors.
With future developments, it may even become possible to intervene before conception, before the genetic determinants of the risk of developing programmed disease are established.”
Table 3 “Antenatal hypoxia and developmental plasticity” column titles were Species | Offspring Phenotypes of Disorders and Diseases | Reference Nos.
This review was really an ebook, with 94 pages and 1,172 citations in the pdf file. As I did with Faith-tainted epigenetics, I read it with caution toward recognizing 1) the influence of the sponsor’s biases, 2) any directed narrative that ignored evidence contradicting the narrative, and 3) any storytelling.
One review topic that was misconstrued was transgenerational epigenetic inheritance of hypoxic effects. The “transgenerational” term was used inappropriately by several of the citations, and no cited study provided evidence for gestational hypoxic effects through the F3 great-grandchild generation.
“One substance that fetuses are frequently exposed to is caffeine, which is a non-selective adenosine receptor antagonist. We discovered that in utero alteration in adenosine action leads to adverse effects on embryonic and adult murine hearts. We find that cardiac A1ARs [a type of adenosine receptor] protect the embryo from in utero hypoxic stress, a condition that causes an increase in adenosine levels.
After birth in mice, we observed that in utero caffeine exposure leads to abnormal cardiac function and morphology in adults, including an impaired response to β-adrenergic stimulation. Recently, we observed that in utero caffeine exposure induces transgenerational effects on cardiac morphology, function, and gene expression.”
The timing of in utero caffeine treatment leads to differences in adult cardiac function, gene expression, and phenotype. Exposure to caffeine from E6.5–9.5 leads the F1 generation to develop dilated cardiomyopathy with decrease % FS and increased Myh7 expression. In utero caffeine exposure from E10.5–13.5 leads to a hypertrophic cardiomyopathy in the F2 generation along with increased % FS and decreased Myh7 expression
Why was this review and its studies omitted? It was on target for both gestational hypoxia and transgenerational epigenetic inheritance of hypoxic effects!
It was alright to review smoking, cocaine, methamphetamine, etc., but the most prevalent drug addiction – caffeine – couldn’t be a review topic?
The Loma Linda review covered a lot, but I had a quick trigger due to the sponsor’s bias. I started to lose “faith” in the reviewers after reading the citation for the review’s last sentence that didn’t support the statement.
My “faith” disappeared after not understanding why a few topics were misconstrued and omitted. Why do researchers and sponsors ignore, misrepresent, and not continue experiments through the F3 generation to produce evidence for and against transgenerational epigenetic inheritance? Where was the will to follow evidence trails regardless of socially acceptable beverage norms?
The review acquired the taint of storytelling with the reviewers’ assertion:
“..timing of the intervention. The greatest potential effect would be accomplished at the critical period in development for which the genomic plasticity is at its peak, thus ameliorating the influence of hypoxia or other stressors.”
Contradictory evidence was in the omitted caffeine study’s graphic above which described two gestational critical periods where an “intervention” had opposite effects, all of which were harmful to the current fetus’ development and/or to following generations. Widening the PubMed link’s search parameters to “caffeine hypoxia” and “caffeine pregnancy” returned links to human early life studies that used caffeine in interventions, ignoring possible adverse effects on future generations.
This is my final curation of any paper sponsored by this institution.
This 2018 Nevada rodent study was on acetyl-L-carnitine’s action in the brainstem:
“We examined age-related changes in the efficiency of synaptic transmission at the calyx of Held, from juvenile adults (1-month old) and late middle-age (18- to 21-month old) mice. The calyx of Held synapse has been exploited as a model for understanding excitation-secretion coupling in central glutamatergic neurons, and is specialized for high-frequency transmission as part of a timing circuit for sound localization.
Our observations suggest that during aging, there is neuronal cell loss in the MNTB [Medial nucleus of the trapezoid body, a collection of brainstem nuclei in an area that’s the first recipient of sound and equilibrium information], similar to previous reports. In remaining synapses of the MNTB, we observed severe impairments in transmission timing and SV [synaptic vesicle] recycling, resulting in timing errors and increased synaptic depression in the calyx of Held synapse. These defects reduce the efficacy of this synapse to encode temporally sensitive information and are likely to result in diminished sound localization.
We orally administered ALCAR for 1 month and found that it reversed transmission defects at the calyx of Held synapse in the older mice.
These results support the concept that facilitators of mitochondrial metabolism and antioxidants may be an extremely effective therapy to increase synaptic function and restore short-term plasticity in aged brains, and provide for the first time a clear mechanism of action for ALCAR on activity-dependent synaptic transmission.“
Human brainstem research is neglected, as noted by Advance science by including emotion in research. Evidence from such research doesn’t play well with beliefs in the popular models and memes of human cerebral dominance.
Do you know any “late middle-age” people who have obvious auditory and synaptic deficits? What if some of the neurobiological causes of what’s wrong in their brains could be “reversed by ALCAR?”
Before using this study as a guide, however, I asked the study’s researchers about the “daily dose of ~2.9 g/kg/d.” An equivalent for a 70 kg human is (2.9 g x 70) x .081 = 16 grams daily, compared with the 500 mg to 1 g dietary supplement dose of acetyl-L-carnitine.
The study’s corresponding coauthor replied:
“This is indeed much larger than that normally consumed by humans via dietary supplementation. We are currently working to determine the effective ‘minimal’ dose of ALCAR and alpha lipoic acid, to better assist guidelines for human application of this supplement.”