Here are my Day 70 measurements* to follow up Our model clinical trial for Changing to a youthful phenotype with broccoli sprouts, which had these findings:

Keep in mind that I’m not in the population represented by the clinical trial sample:
- My chronological age is above their inclusion range;
- My BMI is below their inclusion range; and
- I take supplements and meet other exclusion criteria.
I also didn’t take Day 0 measurements.
June 2019 BMI: 24.8
June 2020 BMI: 22.4
2020 IL-6: 1.0 pg / ml. See Part 2 of Rejuvenation therapy and sulforaphane for comparisons.
2020 C-reactive protein: < 1 mg / l.

2019 and 2020 No biological age measurements. Why aren’t epigenetic clocks standard and affordable?
I’ve made four lifestyle “interventions” since last summer:
- In July 2019 I started to reduce my consumption of advanced glycation end products after reading Dr. Vlassara’s AGE-Less Diet: How a Chemical in the Foods We Eat Promotes Disease, Obesity, and Aging and the Steps We Can Take to Stop It.
- In September I started non-prescription daily treatments of Vitamin D, zinc, and DHEA per clinical trial Reversal of aging and immunosenescent trends.
- Also in September, I started non-prescription intermittent quercetin treatments of Preliminary findings from a senolytics clinical trial.
- I started eating broccoli sprouts every day eleven weeks ago.
1. Broccoli sprouts oppose effects of advanced glycation end products (AGEs) provided examples of Items 1 and 4 interactions.
2. Two examples of Item 2 treatment interactions with Item 4 are in Reversal of aging and immunosenescent trends with sulforaphane:
- “The effects of the combined treatment with BSE [broccoli sprout extract] and zinc were always greater than those of single treatments.” [Zinc and broccoli sprouts – a winning combination]
- “Vitamin D administration decreased tumor incidence and size, and the co-administration with SFN [sulforaphane] magnified the effects. The addition of SFN decreased the activity of histone deacetylase and increased autophagy.”
3. How broccoli sprout compounds may complement three supplements I take was in a 2020 review Central and Peripheral Metabolic Defects Contribute to the Pathogenesis of Alzheimer’s Disease: Targeting Mitochondria for Diagnosis and Prevention:
“The nutrients benefit mitochondria in four ways, by:
- Ameliorating oxidative stress, for example, lipoic acid;
- Activating phase II enzymes that improve antioxidant defenses, for example, sulforaphane;
- Enhancing mitochondrial remodeling, for example, acetyl-l-carnitine; and
- Protecting mitochondrial enzymes and/or stimulating mitochondrial enzyme activities, for example, enzyme cofactors, such as B vitamins and coenzyme Q10 .
In addition to using mitochondrial nutrients individually, the combined use of mitochondrial nutrients may provide a better strategy for mitochondrial protection.”
The review provided a boatload of mitochondrial multifactorial analyses for Alzheimer’s. But these analyses didn’t include effective mitochondrial treatments of ultimate aging causes. I didn’t see evidence of why, after fifteen years of treating mitochondrial effects with supplements, treating one more effect could account for my Week 9 vastly different experiences.
I nod to An environmental signaling paradigm of aging explanations. Its Section 10 reviewed IL-6, C-reactive protein, senescence, and NF-κB in terms of feedback loops, beginning with:
“It is clear that the increasing number of senescent cells depends on the post-adult developmental stage rather than chronological age. The coincidence that these processes result in particular forms of impairment in old age does not seem to be random as it is present in all mammals, and may be causative of many aspects of aging.”
A derived hypothesis: After sufficient strength and duration, broccoli sprout compounds changed my signaling environment, with appreciable effects beginning in Week 9.
I offered weak supporting evidence in Upgrade your brain’s switchboard with broccoli sprouts where a study’s insufficient one week duration of an insufficient daily 17.3 mg sulforaphane dosage still managed to change a blood antioxidant that may have changed four thalamus-brain-area metabolites. For duration and weight comparisons, I doubled my daily amount of broccoli seeds from one to two tablespoons just before Week 6 (Day 35), and from that point onward consumed a estimated 52 mg sulforaphane with microwaving 3-day-old broccoli sprouts every day.
Maybe a promised “In a submitted study, we will report that peripheral GSH levels may be correlated with cognitive functions” will provide stronger evidence? I’m not holding my breath for relevant studies because:
- There wouldn’t be potential payoffs for companies to study any broccoli sprout compound connections with research areas such as aging, migraines, etc. Daily clinically-relevant broccoli sprout dosages can be grown for < $500 a year.
- Sponsors would have to change paradigms, a very-low-probability event. They’d have to explain why enormous resources dedicated to current frameworks haven’t produced effective long-term treatments.
What long-term benefits could be expected if I continue eating broccoli sprouts every day?
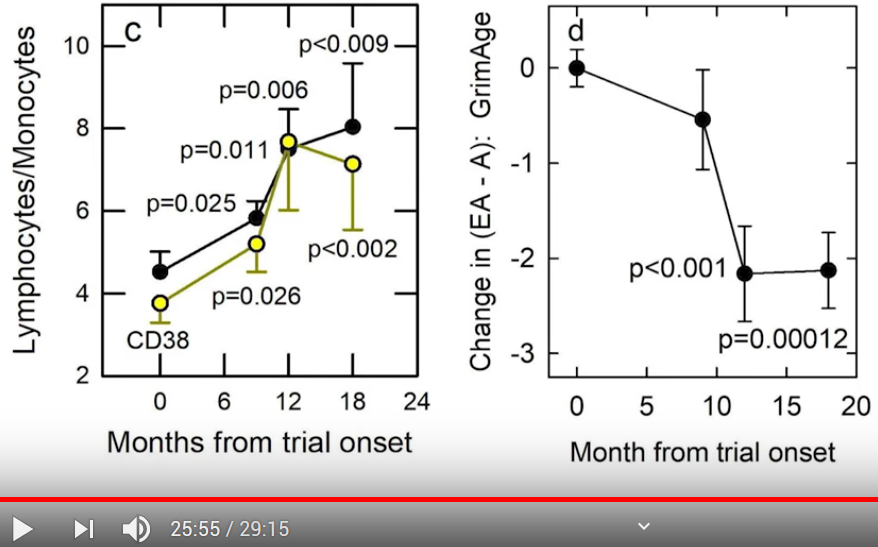
The longest relevant clinical trial I’ve seen – referenced in Part 2 of Reversal of aging and immunosenescent trends with sulforaphane – was twelve weeks. Part 2 also provided epigenetic clock examples of changes measured after 9 months, which accelerated from there to the 12-month end-of-trial point.
Reviewing clinical trials of broccoli sprouts and their compounds pointed out:
“Biomarkers of effect need more time than biomarkers of exposure to be influenced by dietary treatment.”
A contrary argument: Perhaps people don’t require long durations to effectively change their signaling environments?
I apparently didn’t start eating an effective-for-me daily broccoli sprouts dosage until Day 35, when I changed from one to two tablespoons of broccoli seeds a day. If so, Weeks 6 through 8 may account for my substantial responses during Week 9.
- Could eating broccoli sprouts every day for four weeks dramatically change a person’s signaling environment?
- Do you have four weeks and $38 to find out? Two tablespoons of broccoli seeds = 21.4 g x 30 days = .642 kg or 1.42 lbs.
This is what twice-a-day one-tablespoon starting amounts of broccoli seeds look like through three days:

Maintaining the sprouting process hasn’t been a big effort compared with the benefits.
In the absence of determinative evidence, I’ll continue eating broccoli sprouts every day. Several areas of my annual physical have room for improvements. Extending my four lifestyle “interventions” a few more months may also provide hints toward inadequately researched connections.
* Results may not be extrapolatable to other people, to any specific condition, etc.







 Living beings – thousands of years old – living together
Living beings – thousands of years old – living together