To follow up Week 18:
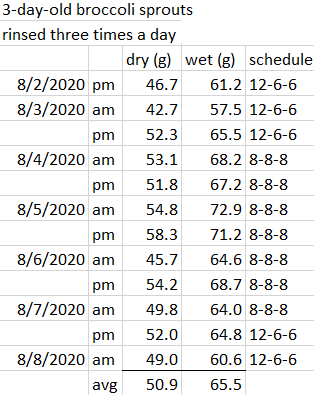
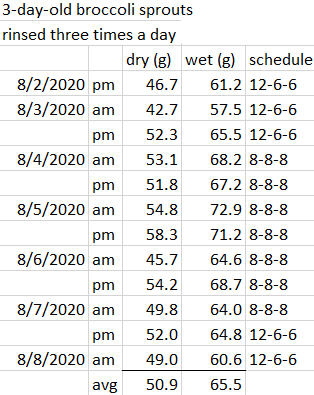
1. Continued attention to broccoli sprout gardening details was this week’s theme. The 12-6-6 schedule had an extra rinse during lunch time.
I stopped when the 8/3 evening batch smelled bad. Broccoli sprouts don’t do well with too much moisture.
I didn’t have this problem on a 12-12 schedule of two rinses. But I also didn’t have good yields.
I switched to an 8-8-8 schedule, and the problem didn’t recur. However, intervals were 5:00 a.m., 1:00 p.m., and 9:00 p.m. That led to eating broccoli sprouts too early and too late, and disrupting my sleep.
8-8-8 also didn’t produce optimal yields. The top two yields this week were both on 8/5. Those two batches started on 8/2, and apparently benefited from a 12-6-6 schedule during their initial germination stages.
I switched back to 12-6-6 on 8/7 with an extra step of rinsing my strainer and teaspoon between batch rinses. Not sure this step addresses whatever happened on 8/3, but it protects against one batch’s problems spreading to other batches. I’ll continue 12-6-6 unless I cause moisture problems, in which case I’ll return to a 12-12 routine.
The (65.5 gram x 2) = 131 g daily average of this week’s broccoli sprouts has been factored into Estimating daily consumption of broccoli sprout compounds numbers for broccoli seeds, sprouts and their compounds. Some worst-case scenarios change to evidenced estimates, such as consuming 52 mg sulforaphane daily by microwaving 131 g of 3-day-old broccoli sprouts.
I’ll update the many blog posts that reference these estimates. Most of them can be recognized from strikethrough typography.
2. During the 8-8-8 schedule I ate microwaved broccoli sprouts with supplements and sauerkraut instead of during a meal. I wondered if meal composition made any difference to broccoli sprout compounds. My meals are breakfast started with 1/2 cup (82 grams) of steel-cut oats, Boring Chicken Vegetable Soup for dinner, and leftover soup at lunch.
A 2018 Netherlands study Bioavailability of Isothiocyanates From Broccoli Sprouts in Protein, Lipid, and Fiber Gels found:
“Compared to the control broccoli sprout, incorporation of sprouts in gels led to lower bioavailability for preformed sulforaphane and iberin.”
IAW, eating protein, fats, and fiber along with microwaved broccoli sprouts wouldn’t help. So I’ll keep eating them with supplements for synergies* but not immediately before or after meals.
A 2018 review with some of the same researchers Isothiocyanates from Brassica Vegetables-Effects of Processing, Cooking, Mastication, and Digestion offered one possible explanation for protein acting to lower broccoli sprout compounds’ bioavailability:
“In vitro studies show that ITCs can potentially react with amino acids, peptides, and proteins, and this reactivity may reduce the ITC bioavailability in protein‐rich foods. More in vivo studies should be performed to confirm the outcome obtained in vitro.”
3. I mix in homemade sauerkraut when I eat microwaved broccoli sprouts. It helps ensure that I thoroughly chew sprouts. Wouldn’t expect anyone else to like unsalted sauerkraut.

Continued with Week 20 of Changing to a youthful phenotype with broccoli sprouts.
*See Broccoli sprout synergies for details.











 Sunrise minus 5 minutes
Sunrise minus 5 minutes