To follow up A rejuvenation therapy and sulforaphane, the study’s lead laboratory researcher – Dr. Harold Katcher – provided evidence for an environmental signaling paradigm of aging in this 2015 paper:
“The age-phenotype of a cell or organ depends on its environment and not its history.
Organ dysfunction is not the cause of aging, but is the result of its milieu. Therefore, the aged milieu is the cause. Though it has been thought that the aging immune system is the cause of aging, it can seen to be the result of aging.
The systemic milieu of an organism sets the age-phenotype of its cells, tissues and organs. Cells and organs secrete factors into blood, which are determined by the age-phenotype and repair-states of those cells and organs. The presence and concentrations of these blood-borne factors determine the age-phenotype of cells and organs.
Here we must be a bit more speculative. Changes in concentrations of factors present in blood, rather than their presence or absence, determines age-phenotype.
Interactions between disparate levels of the body’s hierarchy establish a consensus age-phenotype for cells and organs, and this largely occurs via the bloodstream. There appear to be positive factors that promote youthful age-phenotypes and negative factors that promote the aged phenotypes.
We readily consider development as a ‘program’, and it seems clear that we must consider post-adult development as ‘programmed’ as well. But if there is a program it is neither in genes nor chromatin, but in interaction of complex, interconnected systems spanning hierarchical levels.
If these aforementioned principles are correct, it should be easy to verify. If so, whole organism rejuvenation might require little more than:
- Changing concentrations of all age-determining molecules of the bloodstream and various stem cell niche environments to youthful levels;
- For a time sufficient to cause rejuvenation at the cellular level.
Once cells start secreting factors appropriate to their new, younger age-phenotypes, cognate changes should propagate through hierarchical levels.
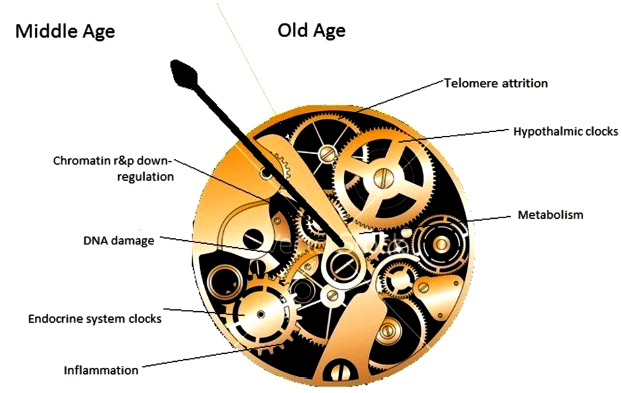
The analogy to workings of a mechanical clock is not very exact. ‘Gears’ represent individual aging clocks, both cellular and organic (shown at different levels within the mechanism) which interact, ultimately resulting in organismic age, i.e. ‘body clock’, represented by the ‘hour hand’ (no minute hand is shown).
In mammals, readout of the clock corresponds to age-related composition of blood plasma. In this model, moving the hour hand backwards should result in a turning back of composite clocks as well – a result obtained when induction to pluripotence is used to reset cellular clocks.
Apart from being slowed down or sped up, the body clock can also be reset. Organisms, organs, and their cells can be reset to different age-phenotypes depending on their environment.
We know that old transplanted tissues and organs can regain function and live for the entire life of the younger host at least in rodents. We must suppose that age-phenotype changes must have taken place at the cellular level to allow this.
Rejuvenation cannot be explained on the basis that aging represents accumulation of irreparable cellular damage.
None of these principles are rigorously established as such, but all are supported by experimental evidence.”
http://www.eurekaselect.com/130538/article “Towards an Evidence-based Model of Aging”
Here are some of his responses to comments on the blog post that first curated his current research:
“We’ve (scientists), spent the past 70 years trying to definitively prove the commonsense ‘wear and tear’ theories and have not succeeded. So I tried something different, looking at results of experiments.
This is not based on ‘theory’ (say mitochondrial aging or ‘wear and tear’) but on experimental evidence. Theory comes in explaining our results, not achieving them. There is a theory becoming clear, one very different from the commonsense view of ‘wear and tear’ aging.
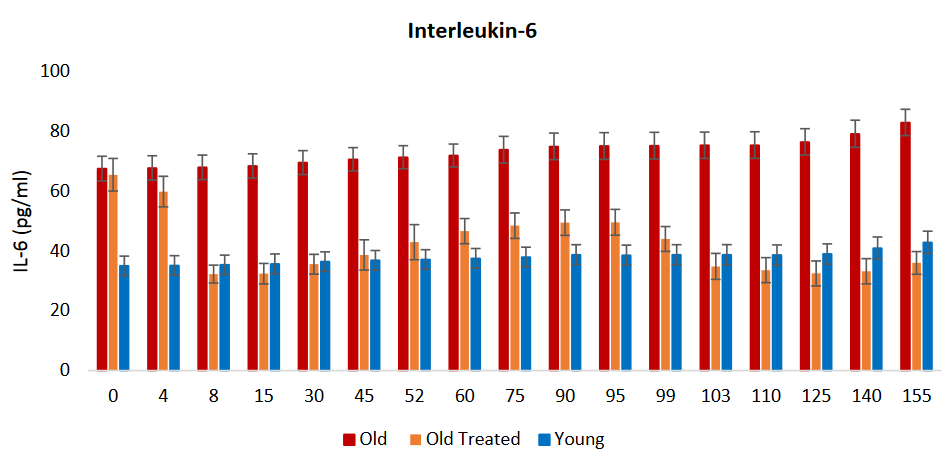
We haven’t examined immune response. All that we know for sure is that chronic inflammation of aging stopped. I can definitively say that chronic inflammation due to aging can be reversed with factors present in young blood.
There are amazing things that Big Pharma won’t touch as there’s not enough profit in them (they can’t be patented). So I guess we’re somewhat the same, but we know what to do and have proven it – for us, it’s not money. However, money allows you to do things.
Being 75 myself puts a time-frame around the project. We plan to propose its use for diseases of aging – eventually, everyone will use it. It will end up changing humanity. As people already seem to have too much free time to begin with, what will people do with those extra years they will be given?”
Sections 3 “Aging Manifestations that Have Hitherto Been Proposed as the Causes of Aging are the Consequences of Aging” and 10 “Several Factors ‘Conspire’ to Promote Inflammation in Old Mammalian Bodies, Inflammation Leads to Several Diseases of Aging and Perhaps to Aging Itself” were especially informative.
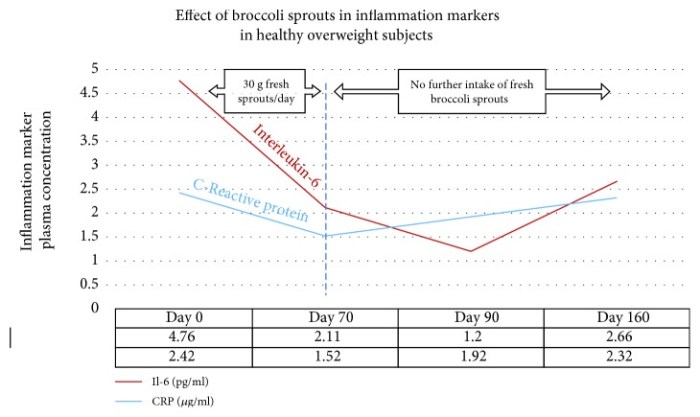
The former section discussed cells that were capable of making repairs but didn’t make repairs, with aging being the consequence of this behavior. The latter reviewed topics such as senescence, IL-6, NF-κB, and C-reactive protein in terms of feedback loops.
See Reevaluate findings in another paradigm for comparisons of Section 6 with another view of hypothalamic aging.