This 2019 Washington rodent study from Dr. Michael Skinner’s lab found adverse effects in the grand-offspring and great-grand-offspring following their ancestor’s exposure during pregnancy to the world’s most commonly used herbicide:
“Using a transient exposure of gestating F0 generation female rats found negligible impacts of glyphosate on the directly exposed F0 generation, or F1 generation offspring pathology. In contrast, dramatic increases in pathologies in the F2 generation grand-offspring, and F3 transgenerational great-grand-offspring were observed.
The transgenerational pathologies observed include prostate disease, obesity, kidney disease, ovarian disease, and parturition (birth) abnormalities:
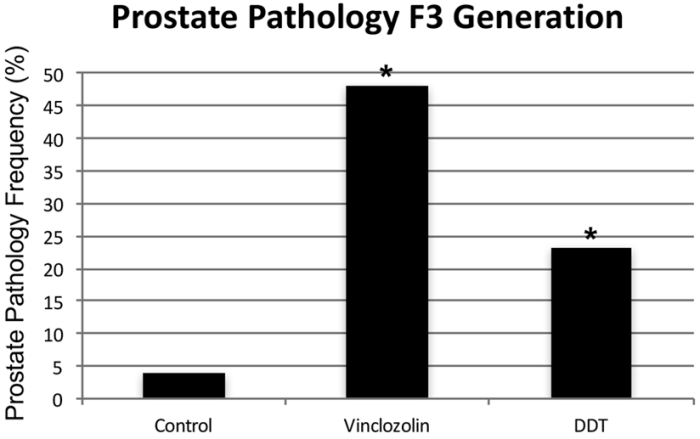
- Prostate disease in approximately 30% of F3 generation glyphosate lineage males, a three-fold increase in disease rate over controls.
- A transgenerational (F3 generation) obese phenotype was observed in approximately 40% of the glyphosate lineage females and 42% of the glyphosate lineage males.
- An increased incidence of kidney disease observed in the F3 generation glyphosate lineage females affecting nearly 40% of females.
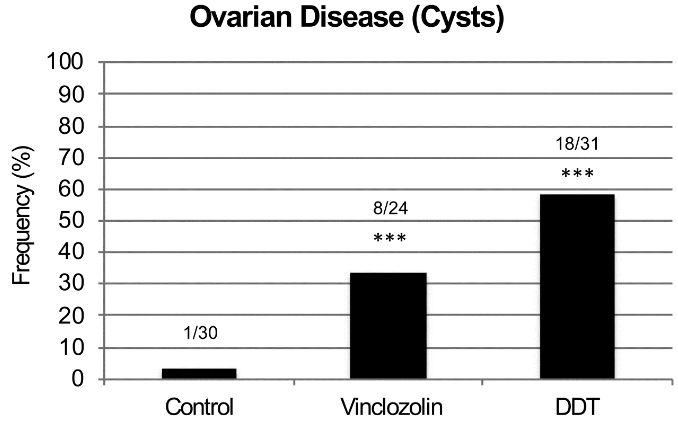
- A significant increase in ovarian disease observed in the F2 [48% vs. 21% for controls] and F3 [36% vs. 15% for controls] generation glyphosate lineage females.
- During the gestation of F2 generation mothers with the F3 generation fetuses, dramatic parturition abnormalities were observed in the glyphosate lineage. The frequency of unsuccessful parturition was 35%. To further investigate the parturition abnormalities an outcross of F3 generation glyphosate lineage males with a wildtype female was performed. There were parturition abnormalities observed with a frequency of 30%.
Classic and current toxicology studies only involve direct exposure of the individual, while impacts on future generations are not assessed. The ability of glyphosate and other environmental toxicants to impact our future generations needs to be considered, and is potentially as important as the direct exposure toxicology done today for risk assessment.”

Why isn’t coverage of this study the top story of world news organizations? Is what’s reported more important than reliable evidence of generational consequences to environmental experiences?
Current toxicology practices are a scientific disgrace:
- What are hypotheses of practices that test only effects on somatic cells, and don’t look for generational effects on germ cells?
- Are tests selected for their relative convenience instead of chosen for their efficacy?
Why don’t sponsors fund and researchers perform human studies of transgenerational epigenetic inheritance? For example, from Burying human transgenerational epigenetic evidence:
“From the late 1930s through the early 1970s, DES was given to nearly two million pregnant women in the US alone.
Fourth [F3] generation effects of prenatal exposures in humans have not been reported.”
Zero studies of probably more than 10,000,000 F3 great-grandchildren of DES-exposed women just here in the US!
There will be abundant human evidence to discover if sponsors and researchers will take their fields seriously.
https://www.nature.com/articles/s41598-019-42860-0.pdf “Assessment of Glyphosate Induced Epigenetic Transgenerational Inheritance of Pathologies and Sperm Epimutations: Generational Toxicology”