This 2018 human study presented the results of 100 patients’ personalized therapies for cognitive decline:
“The first examples of reversal of cognitive decline in Alzheimer’s disease and the pre-Alzheimer’s disease conditions MCI (Mild Cognitive Impairment) and SCI (Subjective Cognitive Impairment) have recently been published..showing sustained subjective and objective improvement in cognition, using a comprehensive, precision medicine approach that involves determining the potential contributors to the cognitive decline (e.g., activation of the innate immune system by pathogens or intestinal permeability, reduction in trophic or hormonal support, specific toxin exposure, or other contributors), using a computer-based algorithm to determine subtype and then addressing each contributor using a personalized, targeted, multi-factorial approach dubbed ReCODE for reversal of cognitive decline.
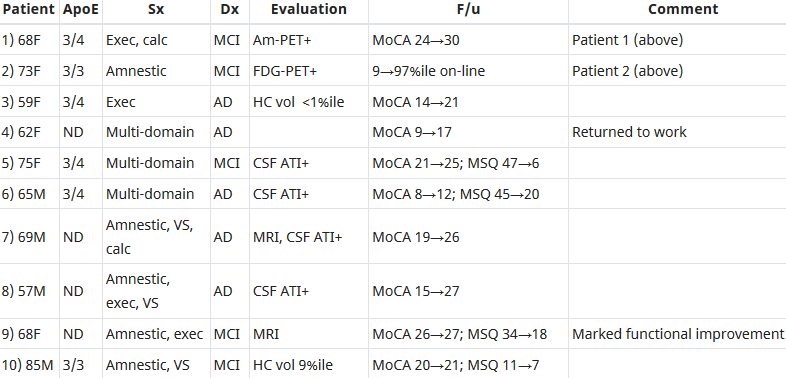
An obvious criticism of the initial studies is the small number of patients reported. Therefore, we report here 100 patients, treated by several different physicians, with documented improvement in cognition, in some cases with documentation of improvement in electrophysiology or imaging, as well.”
https://www.omicsonline.org/open-access/reversal-of-cognitive-decline-100-patients-2161-0460-1000450-105387.html “Reversal of Cognitive Decline: 100 Patients”
The lead author commented on Josh Mitteldorf’s informative post A cure for Alzheimer’s? Yes, a cure for Alzheimer’s!:
- “We have a paper in press, due to appear 10.22.18 (open access, JADP, I’ll send a copy as soon as available), showing 100 patients with documented improvement – some with MRI volumetrics improved, others with quantitative EEG improvements, others with evoked response improvements, and all with quantitative cognitive assessment improvement. Some are very striking – 12 point improvements in MoCA [Montreal Cognitive Assessment], for example – others less so, but all also have subjective improvement. Hopefully this will address some of the criticisms that we haven’t documented improvement in enough people.
- We were just turned down again for a randomized, controlled clinical trial, so on the one hand, we are told repeatedly that no one will believe that this approach works until we publish a randomized, controlled study, and on the other hand, we’ve been turned down (first in 2011/12, and now in 2018), with the complaint that we are trying to address more than one variable in the trial (as if AD is a single-variable disease!). Something of a catch-22. We are now resubmitting (unfortunately, the IRBs are not populated by functional medicine physicians, so they are used to seeing old-fashioned drug studies), and we’ll see what happens.
- I’ve been extending the studies to other neurodegenerative diseases, and it has been impressive how much of a programmatic response there seems to be in these ‘diseases.’
- I agree with you that there are many features in common with aging itself.
- You made a good point that APP [amyloid precursor protein] is a dependence receptor, and in fact it functions as an integrating dependence receptor, responding to numerous inputs (Kurakin and Bredesen, 2015).
- In the book and the publications, we don’t claim it is a “cure” since we don’t have pathological evidence that the disease process is gone. What we claim is ‘reversal of cognitive decline’ since that is what we document.
- As I mentioned in the book, AD is turning out to be a protective response to multiple insults, and this fits well with the finding that Abeta has an antimicrobial effect (Moir and Tanzi’s work). It is a network-downsizing, protective response, which is quite effective – some people live with the ongoing degenerative process for decades.
- We have seen several cases now in which a clinical trial of an anti-amyloid antibody made the person much worse in a time-dependent manner (each time there was an injection, the person would get much worse for 5-10 days, then begin to improve back toward where he/she was, but over time, marked decline occurred), and this makes sense for the idea that the amyloid is actually protecting against pathogens or toxins or some other insult.
- It is important to note that we’ve never claimed that all people get better – this is not what we’ve seen. People very late in the process, or who don’t follow the protocol, or who don’t address the various insults, do not improve. It is also turning out to be practitioner dependent – some are getting the vast majority of people to improve, others very few, so this is more like surgery than old-fashioned prescriptive medicine – you have to do a somewhat complicated therapeutic algorithm and get it right for best results.
- I’m very interested in what is needed to take the next step in people who have shown improvement but who started late in the course. For example, we have people now who have increased MoCA from 0 to 9 (or 0 to 3, etc.), with marked subjective improvement but plateauing at less than normal. These people had extensive synaptic and cellular loss prior to the program. So what do we need to raise the plateau? Stem cells? Intranasal trophic support? Something else?
- I haven’t yet seen a mono-etiologic theory of AD or a mono-therapeutic approach that has repeatedly positive results, so although I understand that there are many theories and treatments, there doesn’t seem to be one etiology to the disease, nor does there seem to be one simple treatment that works for most. It is much more like a network failure.”
At a specific level:
- “There doesn’t seem to be one etiology to the disease,
- Nor does there seem to be one simple treatment that works for most.
- We don’t have pathological evidence that the disease process is gone.”
For general concepts, however:
- “AD is turning out to be a protective response to multiple insults.
- It is a network-downsizing, protective response, which is quite effective.
- The amyloid is actually protecting against pathogens or toxins or some other insult.”
For a framework of an AD cure to be valid, each source of each insult that evoked each “protective response” should be traced.
Longitudinal studies would be preferred inside this framework. These study designs would investigate evidence of each insult’s potential modifying effect on each “protective response” that could affect the cumulative disease trajectory of each individual.
In many cases, existing study designs would be adequate if they extended their periods to the end of the subjects’ natural lifetimes. One AD-relevant example would be extending the prenatally-restraint-stressed model used in:
- Prenatal stress produces offspring who as adults have cognitive, emotional, and memory deficiencies and
- Treating prenatal stress-related disorders with an oxytocin receptor agonist.
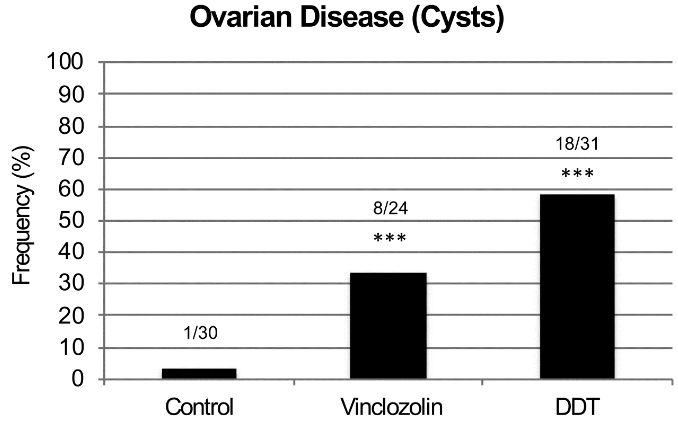
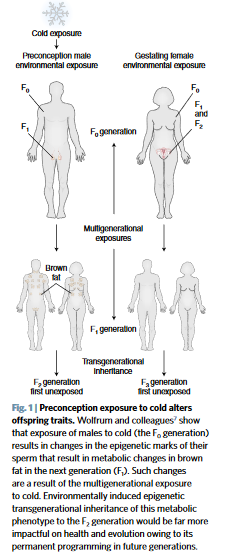
The framework would also encourage extending studies to at least three generations to investigate evidence for transgenerational effects, as were found in: