In this 2014 review, a social scientist first presented an interpretive history of what he found to be important in the emergence of epigenetics. He proceeded into his ideas of “a possible agenda of the social studies of the life-sciences” in the “postgenomic age” with headings such as “Postgenomic biopolitics: “upgrade yourself” or born damaged for ever?”
This perspective included:
“The upgradable epigenome may become the basis for a new motivation to intervene, control and improve it through pharmacological agents or social interventions.
An important trend is the use of epigenetic and developmental findings in the so-called early-intervention programmes.
It is possible that epigenetic findings will become increasingly relevant in social policy strategies.”
In this blog I often highlight research that may help us understand details of how each of us is a unique individual. It’s my view that insofar as research helps each of us understand our unique, real self, we may be able to empathetically understand others’ unique qualities.
Click individual differences for a sample of how researchers explain away uniqueness in order to converge on a study’s desired objectives. There’s seldom an attempt to further understand what caused each subject to develop their unique qualities.
Why would this reviewer advocate that
- Researchers,
- People working in the social sciences,
- People employed or involved in social services, and
- Their sponsors and employers
intentionally disregard another individual’s unique qualities?
I’ll answer this question from a perspective that explains how this common, reflexive action derives from a person being unable to face the facts of their own life. Pertinent fundamentals of Dr Arthur Janov’s Primal Therapy are:
- Pain motivates a person’s unconscious act-outs of their underlying problems.
- The behavior that caused a problem is sometimes also the act-out behavior.
- Act-outs enable a person to re-experience the feelings of their historical struggles, in a vain attempt to resolve them.
- Due to pain barriers, people seldom become consciously aware of and – more importantly – address the causes for their own problematic behavior.
- “The patient has the power to heal himself.”
A consequent hypothesis is that a person will often glorify their unconscious act-outs and surround themself with justifications for these actions. For example, a person who can’t sit still may refer to their incessant activity with socially acceptable phrases such as “I’m always busy” or “I love to travel.” They’ll structure their life to enable their unconscious behavior, never questioning how they were attracted to an always-on-the-go occupation such as flight attendant, only vaguely feeling that they were made for it.
The behavior relevant to the current review may be exhibited by a person with a history of having no control over their own life. Following the above first two fundamentals, the pain of historically not having control over their life may motivate them to control other people’s lives.
Unfortunately for everyone who’s affected, such unconscious act-outs don’t resolve anything:
- The initiator may achieve some symbolic satisfaction by controlling others’ lives.
- This temporary satisfaction doesn’t make the initiator’s underlying problems less painful.
- The motivation impelling these unconscious act-outs isn’t thereby reduced.
- So the initiator soon repeats their controlling behavior, stuck in a loop of unresolved feelings.
- Since the self-chosen interests of someone who’s being controlled are lesser concerns to the initiator than exercising control, the controlled person may or may not be helped by the controller’s act-outs.
Research provides abundant evidence that we are unique individuals.
This is a strong indicator of who is best qualified to direct each of our unique lives.
A person who is driven to control others’ lives won’t accept epigenetic research as instructive for understanding, honoring, and respecting others as unique individuals. They’ll use research as a way to enable their own unconscious act-outs, and view it as offering opportunities for interventions into the lives of others.
This is the way that “pharmacological agents or social interventions” are often the intended “use of epigenetic and developmental findings.” Interventions receive justifications with “a possible agenda of the social studies of the life-sciences.”
Becoming aware of one’s own act-outs – and then individually addressing one’s own underlying problems – often take backseats to employment and other concerns to keep enabling one’s own behavior. That makes it likely that interventions justified by “epigenetic findings..in social policy” will continue, whether or not the subjects agree that they’re being helped.
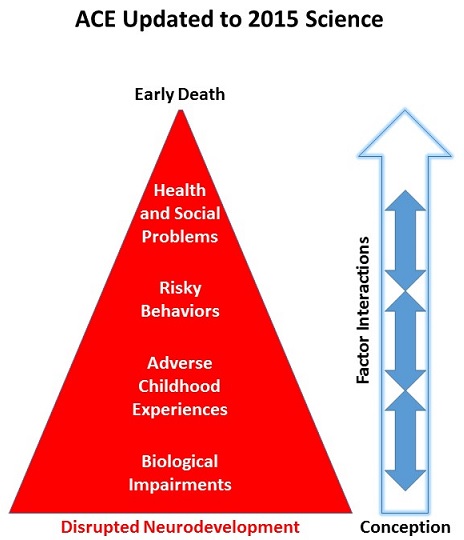
For examples, take a look at a few of the YouTube presentations by people employed in the social sciences and social services on a topic of epigenetics. Compare them with the current state of epigenetic research in Grokking an Adverse Childhood Experiences (ACE) score.
What did you notice? How many presentations emphasized disrupted prenatal development – a period when problems can be prevented? Did you instead see that many more of the presentations emphasized controlling behavior?
http://journal.frontiersin.org/article/10.3389/fnhum.2014.00309/full “The social brain meets the reactive genome: neuroscience, epigenetics and the new social biology“