People will forgive you for being wrong, but they will never forgive you for being right – especially if events prove you right while proving them wrong. Thomas Sowell
A 2026 rodent study investigated sulforaphane’s ability to affect ALS-like symptoms:
“The objective of this study was to evaluate neuroprotective efficacy and safety of sulforaphane (SUFP) in a methylmercury (MMHg⁺)-induced preclinical rat model of amyotrophic lateral sclerosis (ALS). ALS is characterized by progressive motor neuron degeneration and muscle wasting, leading to impairments in gait, swallowing, salivation, and routine motor activities.
64 animals were classified into eight groups: 1st: normal control, 2nd: vehicle control; 3rd: SUFP perse (4 mg/kg, i.p.), 4th: MMHg + (5 mg/kg, p.o.), 5th: MMHg + 5 + SUFP (2 mg/kg, i.p.), 6th: MMHg+ 5 + SUFP (4 mg/kg, i.p.), 7th: MMHg+ 5 + omaveloxolone (OVX) (30 mg/kg, i.p.), and 8th: MMHg + 5 + dimethyl fumarate (DIMT) (50 mg/kg, i.p.). Neurotoxin MMHg + was orally administered at 5 mg/kg for the first 21 days. For the next 22 days, SUFP, OVX, and DIMT were administered intraperitoneally (i.p.).
SUFP modulates neurotransmitter levels such as acetylcholine (A), dopamine (B), GABA (C), glutamate (D), and serotonin (E).
SUFP4 exerted broad neuroprotective effects in ALS pathology by restoring antioxidant proteins (Nrf2, HO-1, SIRT1), suppressing apoptotic (Bax, caspase-3, Bcl-2) and inflammatory markers (TNF-α, IL-1β), and enhancing the anti-inflammatory cytokine IL-10. It also downregulated stress-related signaling pathways (PI3K/Akt, p75NTRECD, MAPKs) associated with neurodegeneration. These molecular effects translated into meaningful functional recovery, as evidenced by improvements in grip strength, locomotor performance, spatial memory, and depressive-like behavior.
Histopathological evaluation demonstrated attenuation of demyelination and preservation of neuronal architecture including the cerebral cortex, hippocampus, striatum, midbrain, and cerebellum. Beyond central neuroprotection, SUFP exerted systemic benefits by normalizing hepatic enzymes, improving skeletal muscle integrity, restoring redox balance, stabilizing neurofilament and myelin-associated proteins, and correcting hematological alterations.
Despite limitations related to study duration and animal sex, this work strongly positions SUFP as a promising, multi-target therapeutic candidate for ALS with both neural and systemic protective efficacy.”
https://link.springer.com/article/10.1007/s12035-026-05683-5 “Sulforaphane-Mediated Multitarget Therapeutic Effects in Methylmercury-Induced ALS-Like Pathology: Comparative Analysis and Multifaceted Approach to Neuroprotection and Systemic Recovery” (not freely available) Thanks to Dr. Sidharth Mehan for providing a copy.
Unlike A Nrf2 treatment for ALS?, this study didn’t present evidence that its treatment compound was effective for preventing ALS. For one thing, currently-known disease factors involving heat shock proteins and associated genes, some of which are Nrf2 targets, weren’t investigated.
Two Nrf2 activators were used in both studies as comparators of Nrf2 activation effects. Neither omaveloxolone nor dimethyl fumarate are ALS causal treatments, though, and have undesirable side effects.
A human equivalent of this study’s higher sulforaphane dose is ((4 mg x .162) x 70 kg) = 45 mg. 45 mg of sulforaphane might be too much to consistently take at one time because of unpalatability. But I documented taking an estimated 52 mg for a year during 2020-2021 by eating microwaved 3-day-old broccoli sprouts twice a day.
Here are five 2025 human ergothioneine studies, starting with a clinical trial of healthy older adults:
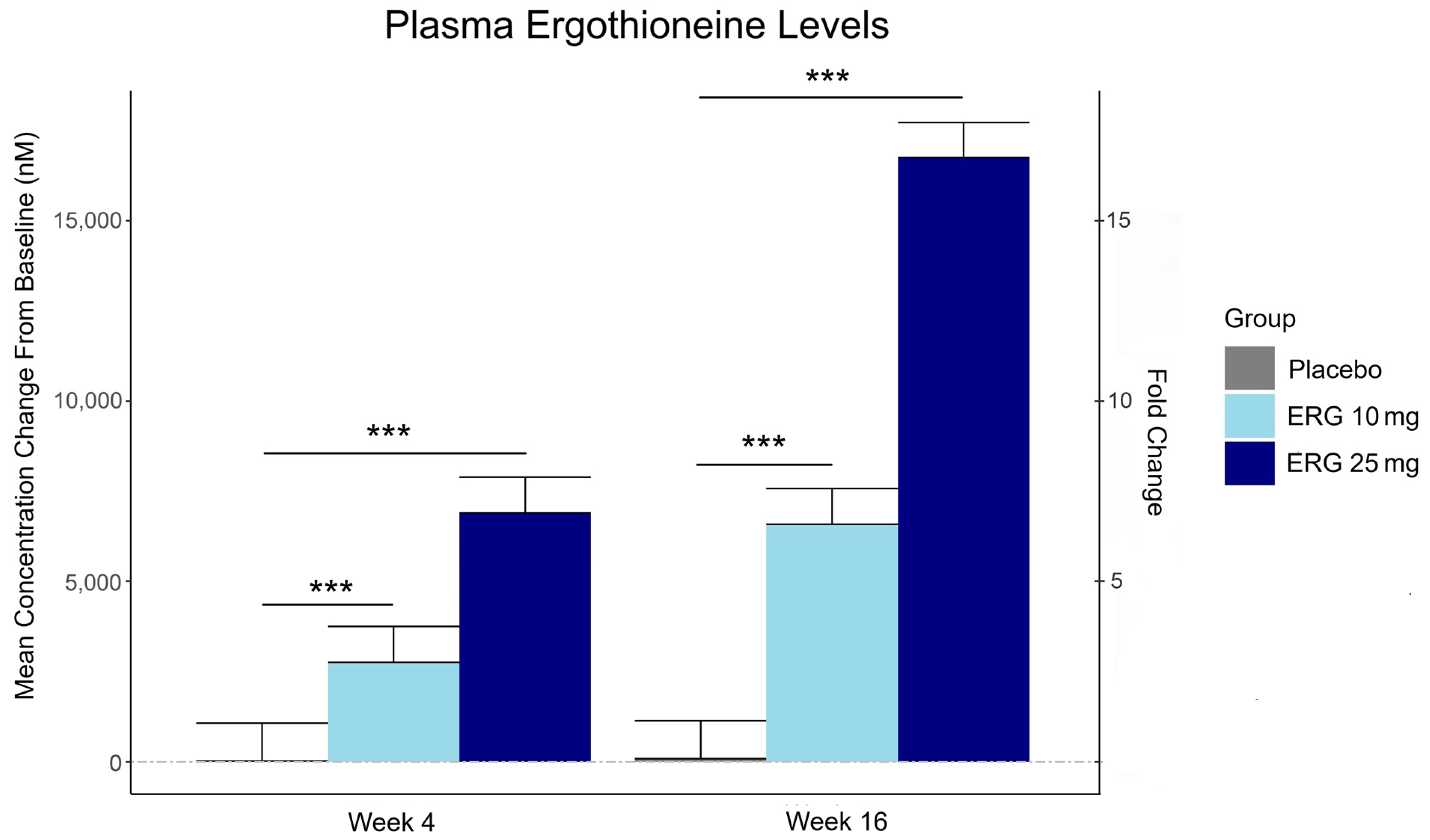
“In this 16-week randomized, double-blind, placebo-controlled trial, 147 adults aged 55–79 with subjective memory complaints received ergothioneine (10 mg or 25 mg/day ErgoActive®) or placebo. Across all the groups, approximately 73% of participants in each group were female, with a median age of 69 years.
The primary outcome was the change in composite memory. Secondary outcomes included other cognitive domains, subjective memory and sleep quality, and blood biomarkers. At baseline, participants showed slightly above-average cognitive function (neurocognitive index median = 105), with plasma ergothioneine levels of median = 1154 nM.
Although not synthesized in the human body, ergothioneine is efficiently absorbed via the OCTN1 transporter (also known as the ergothioneine transporter, or ETT), which is expressed in many tissues, including the intestine, red blood cells, kidneys, bone marrow, immune cells, skin, and brain. This transporter enables ergothioneine to accumulate in high concentrations in organs vulnerable to oxidative stress and inflammation. Ergothioneine has multiple cellular protective functions, including scavenging reactive oxygen species, chelating redox-active metals, suppressing pro-inflammatory signaling, and protecting mitochondrial function.
Plasma ergothioneine increased by ~3- and ~6-fold for 10 mg, and ~6- and ~16-fold for 25 mg, at weeks 4 and 16, respectively.
While the primary outcome, composite memory, showed early improvement in the 25 mg group compared to baseline, this effect was not sustained and did not differ from placebo. Reaction time showed a significant treatment-by-time interaction favoring ergothioneine, yet the between-group differences were not significant, suggesting that any potential benefits were modest and require validation in larger or longer studies.
Other cognitive effects observed were primarily within-group and not consistently dose-responsive, highlighting the challenge of detecting objective cognitive changes over a relatively short study duration in high-functioning healthy populations. However, positive effects of ergothioneine supplementation were observed on subjective measures of prospective memory and sleep initiation that were not seen in the placebo group.
This trial adds to the growing body of evidence supporting the favorable safety profile of ergothioneine. No adverse events attributable to ergothioneine were reported. Additionally, we observed potential hepatoprotective effects, with significant reductions in the plasma AST and ALT levels, particularly among males in the ERG 25 mg group.”
https://www.mdpi.com/1661-3821/5/3/15 “The Effect of Ergothioneine Supplementation on Cognitive Function, Memory, and Sleep in Older Adults with Subjective Memory Complaints: A Randomized Placebo-Controlled Trial”
The third graphic for Ergothioneine dosing, Part 2 showed a human study where a 25 mg dosing stopped after Day 7, but the plasma ergothioneine level stayed significantly higher than baseline through Day 35.
The second graphic for Ergothioneine dosing, Part 2 was a male mouse experiment where plasma ergothioneine levels of a human equivalent 22 mg to 28 mg daily dose kept rising through 92 weeks.
This trial couldn’t explain the desirability of a 25 mg daily dose that was likely (per the second and third graphics for Ergothioneine dosing, Part 2) to sustain the subjects’ increased plasma ergothioneine levels well after the trial ended at Week 16. What effects can be expected from a sustained plasma ergothioneine level that’s 16 times higher than the subjects’ initial levels? Were these 16-fold sustained plasma ergothioneine levels better or worse than the 6-fold increases in the 10 mg group, both of which were likely to continue past the trial’s end?
A representative of the trial’s sponsoring company talked a little more about the trial in this interview:
Another clinical trial investigated ergothioneine’s effects on skin:
“We conducted an 8-week, randomized, double-blind, placebo-controlled clinical trial to evaluate effects of daily oral supplementation with 30 mg of ergothioneine (DR.ERGO®) on skin parameters in healthy adult women aged 35–59 years who reported subjective signs of skin aging. Objective measurements including melanin and erythema indices, skin glossiness, elasticity, and wrinkle and pigmentation counts were used to comprehensively evaluate changes in skin condition.
The OCTN1 transporter is preferentially expressed in basal and granular epidermal layers, where cellular renewal and barrier maintenance are most active. Once internalized, ergothioneine localizes to mitochondria, where it directly scavenges reactive oxygen species (ROS) and protects mitochondrial DNA from UV- and inflammation-induced damage.
At the signaling level, ergothioneine activates key protective pathways such as the Nrf2/ARE axis, enhancing expression of antioxidant enzymes including HO-1, NQO1, and γ-GCLC. These enzymes contribute to redox homeostasis and glutathione regeneration, reinforcing cellular defense systems against photoaging and environmental insult.
In parallel, ergothioneine modulates the PI3K/Akt/Nrf2 and SIRT1/Nrf2 pathways, which are implicated in collagen preservation, inflammation resolution, and mitochondrial maintenance. These pathways converge to reduce matrix metalloproteinase (MMP) activity, enhance collagen synthesis, and suppress pro-inflammatory cytokines (TNF-α, IL-6, IL-1β), all of which are central to maintaining skin structure and function.
Compared to placebo, the DR.ERGO® ergothioneine group showed significantly greater improvements in melanin and erythema reduction, skin glossiness, elasticity, and wrinkle and spot reduction. No adverse events were reported.
These findings corroborate and extend previous clinical evidence from (Hanayama et al., 2024), who investigated an ergothioneine-rich mushroom extract (Pleurotus sp., 25 mg ergothioneine/day) in a 12-week randomized double-blind trial, and (Chunyue Zhang, 2023), who examined pure ergothioneine supplementation (25 mg/day) in a 4-week open-label study. We contextualized our results within this existing literature by comparing key outcomes.
Several limitations should be acknowledged:
The study cohort consisted solely of Japanese women aged 35–59 years, which may limit generalizability across sexes, ethnicities, and age groups.
The 8-week intervention period, while sufficient to detect short-term effects, does not allow conclusions about the sustainability of benefits or the risk of relapse upon discontinuation.
The placebo group also showed modest improvements in self-perception, highlighting the well-documented placebo response in beauty and wellness studies.
This study focused on a single daily dosage (30 mg/day) without evaluating dose–response relationships, and hydration-specific endpoints such as corneometry or transepidermal water loss (TEWL) were not included.”
Two clinical trials investigated ergothioneine’s effects on sleep quality:
“A four-week administration of 20 mg/day ergothioneine (EGT), a strong antioxidant, improves sleep quality; however, its effect at lower doses remains unclear. This study estimated the lower effective doses of EGT using a physiologically based pharmacokinetic (PBPK) model in two clinical trials.
In Study 1, participants received 5 or 10 mg/day of EGT for 8 weeks, and their plasma and blood EGT concentrations were measured. An optimized PBPK model incorporating absorption, distribution, and excretion was assembled. Our results showed that 8 mg/day of EGT for 16 weeks was optimal for attaining an effective plasma EGT concentration.
In Study 2, a randomized, double-blind, placebo-controlled study, participants received 8 mg/day EGT or a placebo for 16 weeks. The subjective sleep quality was significantly improved in the EGT group than in the placebo group.
In mammals, EGT is not generated in the body but is acquired from the diet via the carnitine/organic cation transporter OCTN1/SLC22A4. Its plasma concentration after oral administration is quite stable and gradually increases after repeated dosing on a multi-day basis.
Blood concentrations of EGT increase after Day 8 when EGT intake is interrupted, and they continue to increase until Day 35. The delayed increase in EGT concentration in the blood, compared with that in the plasma, can be interpreted as its efficient uptake by undifferentiated blood cells, which express high levels of OCTN1/SLC22A4 in the bone marrow, and subsequent differentiation to mature blood cells that enter the circulation. This may imply the nonlinear absorption, distribution, and excretion of EGT owing to saturation of the transporter at higher concentrations, potentially leading to difficulty in model construction.
This is the first study to propose a strategy to estimate lower effective doses based on the PBPK model.”
The bolded section above referenced a 2016 study / third graphic for Ergothioneine dosing, Part 2, where a 25 mg dosing stopped after Day 7, but the plasma ergothioneine level stayed high through Day 35. I didn’t see that the referenced 2004 and 2010 studies addressed this 2016 finding.
I also didn’t see that this study’s mathematical model accounted for saturation of the OCTN1 transporter or other effects, such as a very small ergothioneine clearance rate. Okay, lower the ergothioneine dose, and achieve a lower persistent plasma ergothioneine level, to what benefit?
“The present study demonstrated that OCTN1 is associated with myeloid cells rather than lymphoid cells, and especially with erythroid-lineage cells at the transition stage from immature erythroid cells to peripheral mature erythrocytes.”
Persistent high ergothioneine levels aren’t costless. Skewing bone marrow stem cells and progenitor cells toward a myeloid lineage is done at the expense of lymphocytes, T cells, B cells, and other lymphoid lineages.
Where are the studies that examine these tradeoffs? Subjective sleep quality in this study and sleep initiation in the first study above aren’t sufficiently explanatory.
A study investigated associations of plasma ergothioneine levels and cognitive changes in older adults over a two-year period:
“Observational studies have found that lower plasma levels of ergothioneine (ET) are significantly associated with higher risks of neurodegenerative diseases. However, several knowledge gaps remain:
Most of the above studies were based on cross-sectional study design, and potential reverse causation cannot be excluded. It has been suggested that plasma ET declines concomitantly with the deterioration of cognitive function.
Since the impact of a single dietary factor on health is mild, it is prone to be affected by the baseline characteristics of subjects (such as sex, educational level, disease status and gene polymorphism). However, no study has systematically evaluated potential effect modifiers on the association between ET levels and cognitive function.
The dose-response distribution between ET and cognitive function remains undetermined.
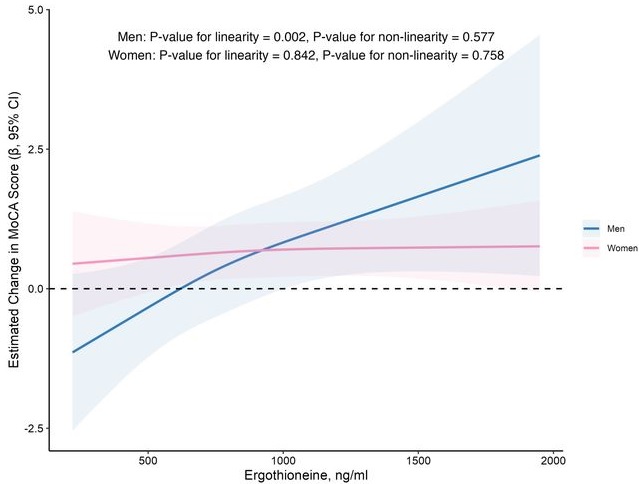
In this prospective cohort study of 1,131 community-dwelling older adults (mean age 69 years), higher baseline plasma ET levels were significantly associated with slower cognitive decline, as assessed by Montreal Cognitive Assessment (MoCA) scores, during a 2-year follow-up period.
When the plasma concentration of ET exceeds 1,000 ng/mL, the decline in cognitive function significantly slows down. However, this association has only been observed in men.
Domain-specific analysis found that the observed ET-MoCA association was mainly driven by the temporary slowdown in the decline of visuospatial/executive and delayed recall. Impaired delayed recall represents one of the earliest and most sensitive cognitive markers of dementia progression, predictive of conversion from MCI to dementia. The preferential preservation of this function by ET suggests targeted neuroprotective effects within the hippocampus.
Visual inspection of the spline curves revealed a potential plateauing effect at ET concentrations ≥1,000 ng/mL in the total population.
Baseline ET concentrations differed between men and women. Most men (81.5%) had concentrations below 1,000 ng/mL (median 754.2, IQR 592.0–937.9 ng/mL). Women exhibited substantially higher median plasma ET concentrations than men, with 35.7% of women exceeded 1,000 ng/mL (median 890.1, IQR 709.7–1,095.6 ng/mL).
Our study included only participants with normal cognitive function, and the results remained robust even after excluding those with baseline cognitive function at the lower end of the normal range. Collectively, our findings support that low ET intake occurs prior to cognitive decline.
Our findings indicate that higher plasma ET levels are significantly associated with slower cognitive decline independent of confounders in non-demented community-dwelling elderly participants, with such association observed in men but not women. Dose-response curves indicated plateauing effects above 1000 ng/mL.”
The average age of this study and the first trial above were both 69 years. Since the first trial’s participants showed slightly above-average cognitive function (neurocognitive index median = 105), with plasma ergothioneine levels of median = 1154 nM at baseline, and this study showed plateauing effects above 1000 ng/mL, I wonder how raising plasma ergothioneine levels above 1000 ng/mL could possibly show a net benefit for older people? What are the trade-offs for older people between potentially increasing slightly above-average cognitive function with ergothioneine and its other effects from saturating their OCTN1 transporter?
This study is at its preprint stage. I’m interested to see if its peer review prompts these researchers to also investigate the common finding that people who are most deficient at baseline have the greatest improvements. If so, would these sex-specific associations still hold?
Wrapping up with a study that investigated associations of serum ergothioneine levels with the risk of developing dementia:
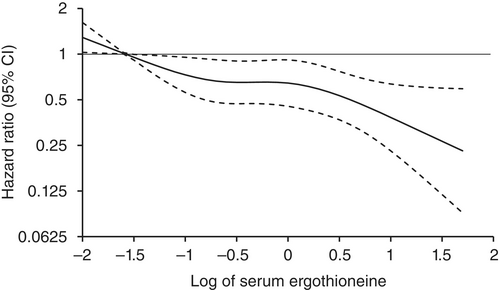
“1344 Japanese community-residents aged 65 years and over, comprising 765 women and 579 men, without dementia at baseline were followed prospectively for a median of 11.2 years.
During follow-up, 273 participants developed all-cause dementia. Among them, 201 had Alzheimer’s disease (AD) and 72 had non-Alzheimer’s disease (non-AD) dementia.
Age- and sex-adjusted hazard ratios (HRs) for all-cause dementia, AD, and non-AD dementia decreased progressively across increasing quartiles of serum ergothioneine. These associations remained significant after adjustment for a wide range of cardiovascular, lifestyle, and dietary factors, including daily vegetable intake.
In subgroup analysis, association between serum ergothioneine levels and the risk of dementia tended to be weaker in older participants and in women:
In older individuals, cumulative burden of multiple risk factors such as hypertension, diabetes mellitus, and smoking may contribute to both neurodegenerative and vascular pathology, potentially diminishing the relative influence of ergothioneine.
In women, postmenopausal hormonal changes, particularly the decline in estrogen, have been associated with increased oxidative stress and a higher vulnerability to neurodegenerative changes.
Several limitations should be noted:
Since serum ergothioneine levels and other risk factors were measured only at baseline, we could not evaluate the changes of serum ergothioneine levels during the follow-up period. Lifestyle modifications during follow-up could have influenced serum ergothioneine levels and other risk factors. In addition, serum ergothioneine level was measured only once, and from a sample.
We cannot rule out residual confounding factors, such as other nutrients in mushrooms and socioeconomic status.
There is a possibility that dementia cases at the prodromal stage were included among participants with low serum ergothioneine levels at baseline.
We are unable to specify which mushroom varieties were predominantly consumed by participants in the town of Hisayama.
Given the limited discriminative ability of serum ergothioneine and potential degradation due to long-term sample storage, we were unable to explore a clinically meaningful threshold value of serum ergothioneine.
Generalizability of findings was limited because participants of this study were recruited from one town in Japan.
These findings suggest that the potential benefit of ergothioneine may be attenuated in individuals with pre-existing, multifactorial risk profiles for dementia.
Our findings showed that higher serum ergothioneine levels were associated with a lower risk of developing all-cause dementia, AD, and non-AD dementia in an older Japanese population. Since ergothioneine cannot be synthesized in the human body, a diet rich in ergothioneine may be beneficial in reducing the risk of dementia.”
For five years I got most of my estimated 7 mg daily ergothioneine intake from mushrooms in AGE-less chicken vegetable soup per Ergothioneine dosing. The soup was always boring, but I got too bored this year and stopped making it. I haven’t replaced mushroom intake with supplements.
I still don’t eat fried or baked foods, preferring sous vide and braising cooking methods to avoid exogenous advanced glycation end products. I avoid buying foods that evoke a hyperglycemic response or otherwise form excessive endogenous AGEs per All about AGEs.
A 2025 rodent study compared protective effects of sulforaphane and a migraine compound on nitroglycerin-induced migraines:
“Activation of trigeminal vascular pathways and the release of calcitonin gene‐related peptide (CGRP) are central to migraine pathogenesis. The amylin‐1 (AMY1) receptor is expressed in key structures implicated in migraine mechanisms.
This study evaluated protective effects of sulforaphane (SFN) against nitroglycerin induced migraine in female mice, comparing its efficacy to the standard migraine medication, topiramate. Migraine was induced using nitroglycerin (10 mg/kg, i.p., administered every other day), and treatments included sulforaphane (5 mg/kg/day, i.p.) or topiramate (30 mg/kg/day, i.p.) for a duration of 9 days.
Sulforaphane demonstrated significant improvements in behavioral symptoms such as photophobia, head grooming, and both mechanical and thermal allodynia. These behavioral changes were accompanied by reductions in serum levels of nitric oxide, CGRP, and pro‐inflammatory cytokines.
Histological analysis revealed that sulforaphane ameliorated nitroglycerin-induced damage in the trigeminal ganglia and trigeminal nucleus caudalis. Additionally, sulforaphane reduced AMY1 receptor expression in the medulla and inhibited its downstream signaling components, including phosphorylated ERK1/2, P38, and c‐Fos. Sulforaphane further enhanced the Nrf2/HO‐1 pathway while suppressing the NF‐κB/NLRP3/caspase‐1 signaling cascade.
These findings indicate that SFN has a potential as a novel therapeutic candidate for migraine management by targeting the downstream signaling pathways of the AMY1 receptor.”
“AMD progression from intermediate to late AMD leads to a point of irreversible retinal pigmented epithelium (RPE) degeneration where treatment becomes worthless. Treating patients at the early/intermediate stages presents a better therapeutic window opportunity for AMD as the disease could potentially be prevented or slowed down.
Strong evidence points to RPE dysfunction at these stages, mainly through redox imbalance and lysosomal dysfunction in RPE oxidative injury. Restoring oxidative balance and lysosomal function may act as preventive and therapeutic measures against RPE dysfunction and degeneration.
Due to interaction with KEAP1, NRF2 is a ubiquitously expressed protein with a high turnover and half-life of about 20 minutes. Because the turnover of NRF2 is faster than KEAP1, newly synthesized NRF2 does not have free KEAP1 to bind and is translocated into the nucleus. Once in the nucleus, NRF2 dimerizes with sMAF and the complex binds to antioxidant response element (ARE) sequences, promoting the expression of ARE genes.
There is NRF2 involvement in most of the hallmarks of aging. Key transcriptional regulatory factors of related pathways, such as transcription factor EB (TFEB) and NRF2, may be targeted to restore homeostasis and/or prevent further RPE degeneration.”
There were other informative tidbits throughout this review, such as:
“Anti-inflammatory effects of most electrophilic NRF2 activators are thought to be at least partly NRF2-independent, suggesting that these compounds lacking specificity may be advantageous for multitargeted pathologies.
TFEB can activate NRF2 under conditions devoid of oxidative stress.”
In this human cell and rodent study, several coauthors of the original 2020 study tested sulforaphane and TFEB interactions for ameliorating effects of a rare disease:
“Mutations in genes encoding lysosomal proteins could result in more than approximately 70 different lysosomal storage disorders. Niemann–Pick disease type C (NPC) is a rare lysosomal storage disorder caused by mutation in either NPC1 or NPC2 gene. Deficiency in NPC1 or NPC2 protein results in late endosomal/lysosomal accumulation of unesterified cholesterol.
Clinical symptoms of NPC include hepatosplenomegaly, progressive neurodegeneration, and central nervous system dysfunction, that is, seizure, motor impairment, and decline of intellectual function. So far there is no FDA-approved specific therapy for NPC.
Under stress conditions, that is, starvation or oxidative stress, TFEB is dephosphorylated and actively translocates into the nucleus, promoting expression of genes associated with lysosome and autophagy. TFEB overexpression or activation results in increased number of lysosomes, autophagy flux, and exocytosis.
Pharmacological activation of TFEB by sulforaphane (SFN), a previously identified TFEB agonist, significantly promoted cholesterol clearance in human and mouse NPC cells, while genetic inhibition (KO) of TFEB blocked SFN-induced cholesterol clearance. This clearance effect exerted by SFN was associated with upregulated lysosomal exocytosis and biogenesis. SFN treatment has no effect on the liver and spleen enlargement of Npc1 mice.
SFN is reportedly BBB-permeable, assuring a good candidate for efficient delivery to the brain, which is essential for targeting neurodegenerative phenotypes in neurological diseases including NPC. This is the first time that SFN was shown to directly activate TFEB in the brain.
Collectively, our results demonstrated that pharmacological activation of TFEB by a small-molecule agonist can mitigate NPC neuropathological symptoms in vivo. TFEB may be a putative target for NPC treatment, and manipulating lysosomal function via small-molecule TFEB agonists may have broad therapeutic potential for NPC.”
https://elifesciences.org/articles/103137 “Small-molecule activation of TFEB alleviates Niemann–Pick disease type C via promoting lysosomal exocytosis and biogenesis”
A 2025 review subject was sulforaphane and brain health. This paper was the latest in a sequence where the retired lead author self-aggrandized his career by citing previous research.
He apparently doesn’t personally do what these research findings suggest people do. The lead author is a few weeks older than I am, and has completely white hair per an interview (Week 34 comments). I’ve had dark hair growing in (last week a barber said my dark hair was 90%) since Week 8 of eating broccoli sprouts every day, which is a side effect of ameliorating system-wide inflammation and oxidative stress.
If the lead author followed up with what his research investigated, he’d have dark hair, too. Unpigmented white hair and colored hair are both results of epigenetics.
Contrast this lack of personal follow-through of research findings with Dr. Goodenowe’s protocol where he compared extremely detailed personal brain measurements at 17 months and again at 31 months. He believes enough in his research findings to personally act on them, and demonstrate to others how personal agency can enhance a person’s life.
It’s every human’s choice whether or not we take responsibility for our own one precious life. I’ve read and curated on this blog many of this paper’s references. Five years ago for example:
An excerpt from the latest video at Dr. Goodenowe’s Health Matters podcast, Episode 7 “The Truth about Parkinson’s”, starting at 50:30:
“What’s exciting about this community medicine focus that we’ve switched to which basically says: How do we develop technologies in a way that they can be incorporated into a community model versus a pharmaceutical drug model? People can actually do I would say self-experiment just the way you self-experiment with your own diet because these are fundamentally dietary nutrition molecules.
Could you give me an elevator pitch because there are probably people listening who are thinking what is this plasmalogen precursor and for sure how is it having this dramatic effect?
Plasmalogens are the most important nutrient that nobody knows about. Normally you don’t know about it because the body is usually pretty good at making them. What makes plasmalogens unique is that your body makes them kind of like cannon fodder, the first group of people that go into war. Your body throws them out for destruction. They absorb oxidative stress and get destroyed in the process.
They’re stored in your cell membranes. 50% of the membranes of your heart are these plasmalogen molecules. When your heart gets inflamed, what your heart does is it dumps these plasmalogens out of its membranes to douse the flame of inflammation. After inflammation is under control, your body naturally builds these things back up again.
But if you have an inability to make enough plasmalogens, these inflammation events knock you down and keep you down. So plasmalogen precursors are critical for maintaining high levels of plasmalogens across your body, not just in your brain (30% of the lipids in your brain) but in your heart, your lungs, your kidneys.”
This September 2024 presentation adds data points and concepts to Part 1:
“Your brain is dynamically connected to and adaptivelyresponsive to its environment.
You are in control of this environment (nutrition, stimulation, adversity).
Need to measure the environment (lab testing, physiology) and adaptive response to the environment (MRI) to optimize your environment (nutrition, lifestyle) to achieve optimal brain structure, function, health, and longevity.
From a global cortical volume and thickness perspective, 17 months of high dose plasmalogens reversed about 15 years of predicted brain deterioration. 31 months reversed almost 20 years. So you can get more out of life.”
Dr. Goodenowe also added case studies of two patients:
1. A 50-year-old woman with MS who had been legally blind in one eye for 32 years who regained sight in that eye after eight months of supplementation.
“This is the adaptability of the human brain. Her eye is not actually impaired. What’s impaired is the ability, the adaptability of the brain to the signal of light, to actually start interpreting what that light signal is.”
2. A 61-year-old man with dementia from firefighting work for the U.S. Navy in a toxic environment with head injuries after nine months of supplementation.
“The brain can heal itself is the point of the story. His executive function skills in everyday life are getting better.”
A 2024 primate study investigated effects of an off-patent drug on age-related changes:
“We evaluated geroprotective effects of metformin on adult male cynomolgus monkeys. The study encompassed a comprehensive suite of physiological, imaging, histological, and molecular evaluations, substantiating metformin’s influence on delaying age-related phenotypes at the organismal level.
Results highlighted a significant slowing of aging indicators, notably a roughly 6-year regression in brain aging. Metformin exerts a substantial neuroprotective effect, preserving brain structure and enhancing cognitive ability.
Geroprotective effects on primate neurons were partially mediated by activation of Nrf2, a transcription factor with anti-oxidative capabilities.”
“Metformin treatment resulted in increased nuclear phosphorylated Nrf2, accompanied by up-regulation of Nrf2 target genes like HO-1, NQO-1, SOD3, GPX2, and GPX1, which were generally suppressed and typically down-regulated during human neuron senescence.
Genes pivotal for neuronal function, such as dendrite morphogenesis/extension and synapse assembly (e.g., GSK3B, GRID2, and NRG3), were down-regulated during aging in excitatory neurons (ExN), inhibitory neurons (InN), oligodendrocytes (OL), oligodendrocyte progenitor cells (OPC), microglia, and astrocyte but were restored by metformin treatment. By contrast, pathways that were up-regulated during aging, including activation of the immune response, complement activation, and regulation of the TGF-b receptor signaling pathway, were reset to lower levels by metformin treatment.
We verified that markers associated with brain aging and progression of neurodegenerative diseases were restored by metformin treatment to levels similar to those observed in young monkeys. Additionally, we observed that reduced myelin sheath thickness, a characteristic of aged monkeys, was rebuilt to a younger state following metformin treatment.
These findings align with the levels of nuclear-localized phosphorylated Nrf2, suggesting that Nrf2 pathway activation is a key mechanism in metformin’s role in delaying human neuronal aging and, by extension, brain aging. Consistent with our in vitro findings, Nrf2 pathway activation was also detected across multiple tissues in metformin-treated monkeys, including frontal lobe neurons.
At last count, I’ve curated 250+ papers this decade on cruciferous vegetables, and many of these explored relationships with Nrf2 activation. Basically, eating a clinically-relevant daily dose of 3-day-old cruciferous sprouts and taking off-patent metformin both induce Nrf2 activation effects.
Don’t expect to see many researchers highlighting this equivalency. They’d rather wait another decade to nitpick other studies with not-enough-subjects / not-exactly replicated / other nitpicks before expressing opinions urging caution from their nursing home beds.
But even then, they won’t get their facts straight. For example, a contemporaneous opinion article https://www.nature.com/articles/d41586-024-02938-w “The brain aged more slowly in monkeys given a cheap diabetes drug” attempted to summarize this study, and flubbed two points:
1. The study said: “We conducted a proof-of-concept study involving male cynomolgus monkeys (Macaca fascicularis) aged between 13 and 16 years, roughly equivalent to approximately 40–50 years in humans. Monkeys adhered to this regimen for a period of 1,200 days, approximately 3.3 years, which corresponds to about 10 years in humans.”
The opinion claimed: “Animals took the drug for 40 months, which is equivalent to about 13 years for humans.”
2. The opinion quoted a New York City researcher involved in a separate metformin study and employed at a medical school for:
“Research into metformin and other anti-ageing candidates could one day mean that doctors will be able to focus more on keeping people healthy for as long as possible rather than on treating diseases.”
This statement is a big break from the realities of medical personnel daily actions at least so far this decade, which is when I started to pay close attention:
Doctors have very little diet and exercise training in medical school. There’s no way they can give health advice. There’s no way that a “keeping people healthy”paradigm will emerge from the current medical system.
Fixing a disease doesn’t restore a patient’s health. Dr. (PhD) Goodenowe cites several examples in his talks, such as a study that compared colorectal cancer therapy with post-operation patient health.
If you listen to yesterday’s two-hour-long podcast, the currently injured person in the first hour gave plenty of contrary evidence of doctors’ focuses: behaviors of trying to blame and gaslight the patient, thinly-disguised punitive actions, CYA etc., all of which they will be sued for one day. The doctor in the second hour provided an example of the quoted researcher in her explanation of how doctors higher in the hierarchy either can’t see or can’t admit realities of doctor/patient interactions, and what therapies have actually benefited or harmed a patient.
Three papers on myelin and oligodendrocytes, starting with a 2023 review:
“Myelin is the spiral ensheathment of axons by a lipid and cholesterol-rich glial cell membrane that reduces capacitance and increases resistance of the axonal membrane. Axonal myelination speeds up nerve conduction velocity as a function of axon diameter.
While myelination proceeds rapidly after birth in the peripheral nervous system, central myelination is a spatially and temporally more regulated process. Ongoing myelination of the human brain has been documented at up to 40 years of age. This late myelination in the adult cortex is followed by exhaustion of oligodendrocyte precursor cells (OPC) with senescence and a gradual loss of myelin integrity in the aging brain.
The brain is well known for its high energy demands, specifically in gray matter areas. In white matter tracts, energy consumption is lower. Myelination poses a unique challenge for axonal energy generation where myelin sheaths cover more than 95% of the axonal surface areas.
Oligodendrocytes help support axonal integrity. Oligodendrocytes survive well in the absence of mitochondrial oxidative phosphorylation, and without signs of myelin loss, cell death, neurodegeneration or secondary inflammation.
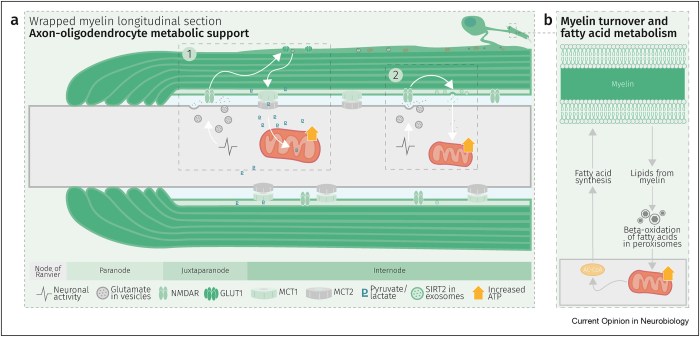
Glycolysis products of oligodendroglial origin are readily metabolized in axonal mitochondria. Oligodendroglial metabolic support is critical for larger and faster-spiking myelinated axons that also have a higher density of mitochondria. An essential requirement for the direct transfer of energy-rich metabolites from oligodendrocytes to the myelinated axonal compartment is ‘myelinic channels’ within the myelin sheath.
Interactions of oligodendrocytes and myelin with the underlying axon are complex and exceed the transfer of energy-rich metabolites. Continuous turnover of myelin membranes by lipid degradation and fatty acid beta-oxidation in mitochondria and peroxisomes leads to recycling of acetate residues by fatty acid synthesis and membrane biogenesis.
In human multiple sclerosis (MS) and its animal model myelin oligodendrocyte glycoprotein-experimental autoimmune encephalomyelitis (MOG-EAE), acute inflammatory demyelination is followed by axonal degeneration in lesion sites that is mechanistically not fully understood. It is widely thought that demyelination and the lack of an axon-protective myelin sheath in the presence of numerous inflammatory mediators are the main causes of axon loss.
But unprotected axons improve rather than worsen the overall clinical phenotype of EAE mice which exhibited the same degree of autoimmunity. Thus, ‘bad myelin is worse than no myelin’ because MS-relevant myelin injuries perturb the integrity of myelinic channels and metabolic support.
Dysfunctional or injured oligodendrocytes that do not allow for compensation by any other cell types turn the affected myelin ensheathment into a burden of the underlying axonal energy metabolism, which causes irreversible axon loss. Any loss of myelin integrity, as seen acutely in demyelinating disorders or more gradually in the aging brain, becomes a risk factor for irreversible neurodegeneration.”
A 2024 review focused on myelin and oligodendrocyte plasticity:
“This review summarizes our current understanding of how myelin is generated, how its function is dynamically regulated, and how oligodendrocytes support the long-term integrity of myelinated axons.
Apart from its unique ultrastructure, there are several other exceptional features of myelin. One is certainly its molecular composition. Another is its extraordinary stability. This was compellingly illustrated when 5000-year-old myelin with almost intact ultrastructure was dissected from a Tyrolean Ice Man.
Myelin is a stable system in contrast to most membranes. However, myelin is compartmentalized into structurally and biochemically distinct domains. Noncompacted regions are much more dynamic and metabolically active than tightly compacted regions that lack direct access to the membrane trafficking machinery of oligodendrocytes.
The underlying molecular basis for stability of myelin is likely its lipid composition with high levels of saturated, long chain fatty acids, together with an enrichment of glycosphingolipids (∼20% molar percentage of total lipids) and cholesterol (∼40% of molar percentage of total lipids). In addition, myelin comprises a high proportion of plasmalogens (ether lipids) with saturated long-chain fatty acids. In fact, ∼20% of the fatty acids in myelin have hydrocarbon chains longer than 18 carbon atoms (∼1% in the gray matter) and only ∼6% of the fatty acids are polyunsaturated (∼20% in gray matter).
With maturation of oligodendrocytes, the plasma membrane undergoes major transformations of its structure. Whereas OPCs are covered by a dense layer of large and negatively charged self-repulsive oligosaccharides, compacted myelin of fully matured oligodendrocytes lacks most of these glycoprotein and complex glycolipids.
Schematic depiction of an oligodendrocyte that takes up blood-derived glucose and delivers glycolysis products (pyruvate/lactate) via monocarboxylate transporters (MCT1 and MCT2) to myelinated axons. Oligodendrocytes and myelin membranes are also coupled by gap junctions to astrocytes, and thus indirectly to the blood–brain barrier.
Adaptive myelination refers to dynamic events in oligodendroglia driven by extrinsic factors such as experience or neuronal activity, which subsequently induces changes in circuit structure and function. Understanding how these adaptive changes in neuron-oligodendroglia interactions impact brain function remains a pressing question for the field.
Transient social isolation during adulthood results in chromatin and myelin changes, but does not induce consequent behavioral alterations. When mice undergo a social isolation paradigm during early life development, they similarly exhibit deficits in prefrontal cortex function and myelination, but these deficiencies do not recover with social reintroduction. This implicates a critical period for social deprivation effects on myelin dynamics. Experience-dependent changes in myelin dynamics may depend on not only the age, brain region, and cell type studied, but also the specific myelin structural change assessed.
Local synaptic neurotransmitter release along an axon not only affects the number of OPCs and oligodendrocytes associated with that axon and local synthesis of myelin proteins, but also drives preferential selection of active axons for myelination over the ensheathment of electrically silenced neighboring axons. Neuronal activity–induced plasticity may preferentially impact brain regions that remain incompletely myelinated compared to more fully myelinated tracts.
Whereas the myelin sheath has been regarded for a long time as an inert insulating structure, it has now become clear that myelin is metabolically active with cytoplasmic-rich pathways, myelinic channels, for movement of macromolecules into the periaxonal space. The myelin sheath and its subjacent axon need to be regarded as one functional unit, which are not only morphological but also metabolically coupled.”
A 2024 rodent study investigated oligodendrocyte precursor cell transcriptional and epigenetic changes:
“We used single-cell RNA sequencing (scRNA-seq), single-cell ATAC sequencing (scATAC-seq), and single-cell spatial transcriptomics to characterize murine cortical OPCs throughout postnatal life. One group (active, or actOPCs) is metabolically active and enriched in white matter. The second (homeostatic, or hOPCs) is less active, enriched in gray matter, and predicted to derive from actOPCs. Relative to developing OPCs, both actOPCs and hOPCs are less active metabolically and have less open chromatin.
In adulthood, these two groups are transcriptionally but not epigenetically distinct, indicating that they may represent different states of the same OPC population. If that is the case, then one model is that the parenchymal environment maintains adult OPCs within an hOPC state, whereas those OPCs recruited into white matter or exposed to demyelinated axons may transition toward an actOPC state in preparation for making new oligodendrocytes. We do not yet know the functional ramifications of these differences, but this finding has clear implications for the development of therapeutic strategies for adult remyelination.
Another finding is that developing but not adult actOPC chromatin is preferentially open for binding motifs associated with neural stem cells, transit-amplifying precursors, and neurogenesis. Although this may simply reflect their origin as the immediate progeny of neonatal neural precursor cells, it may also explain why developing but not adult OPCs have the capacity to make neurons in culture.
If we could, at least in part, reverse the global chromatin shutdown that occurs between development and adulthood, then perhaps adult OPCs may reacquire the ability to make neurons or become better able to generate new oligodendrocytes for remyelination.”
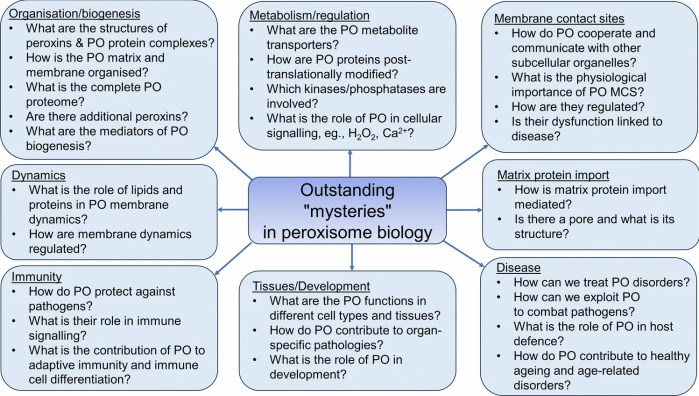
A 2024 review provided details about “mysteries” in peroxisome research:
“Peroxisomes are key metabolic organelles with essential functions in cellular lipid metabolism (e.g., β-oxidation of fatty acids and synthesis of ether phospholipids, which contribute to myelin sheath formation), and metabolism of reactive oxygen species (ROS), particularly hydrogen peroxide. Loss of peroxisomal function causes severe metabolic disorders in humans.
Additional non-metabolic roles of peroxisomes have been revealed in cellular stress responses, regulation of cellular redox balance and healthy ageing, pathogen and antiviral defence, and as cellular signalling platforms. New findings also point to a role in regulation of immune responses.
In our previous reviews, we addressed the role of peroxisomes in the brain, in neurological disorders, in development of cancer, and in antiviral defence. To avoid repetition, we refer to those articles where appropriate, and to more specialised recent reviews on peroxisome biology.
Proper functioning of peroxisomes in metabolism requires the concerted interaction with other subcellular organelles, including the endoplasmic reticulum (ER), mitochondria, lipid droplets, lysosomes, and the cytosol. A striking example of peroxisome-ER metabolic cooperation is de novo biosynthesis of ether phospholipids.
Metabolic activities of peroxisomes, such as ɑ- and β-oxidation of fatty acids, plasmalogen synthesis, and ROS/reactive nitrogen species metabolism, have been linked to numerous immune-related pathways. Roles for peroxisomes in immune and defence mechanisms have opened a new field of peroxisome research, and highlight once more how important peroxisomes are for human health and disease.
It is still not fully understood how peroxisomal functions and abundance are regulated, what kinases/phosphatases are involved, or how peroxisomes are linked to cellular signalling pathways and how they act as signalling platforms.”
Last Friday was Day 90 of a 90-day trial of plasmalogens coincident with improving peroxisomal function via resistance exercise and time-restricted eating. A sticking point has been leg resistance exercises. Ankle issues are interfering with progress, although beach walks aren’t similarly affected. I’m almost back to an upper body exercise routine of five years ago, and I’ve added a half-dozen abs exercises.
I’ll continue taking the two Prodrome plasmalogen precursor supplements (ProdromeGlia and ProdromeNeuro) and with efforts to improve peroxisomal function. Since achieving effective resistance exercise levels is taking longer than expected, and my crystal ball is out-of-commission, I don’t have a realistic end time estimate for stopping the supplements.
A webinar from earlier this week with Dr. Goodenowe, a clinical trial facilitator, and a physician:
From the Q&A segment:
“Is there a particular age where it’s recommended to test for plasmalogen levels? And what levels would be considered normal?
That’s a good question. That actually raises this whole concept of optimal health and this concept of aging.
The best way to think about it – we talked about this paycheck-to-paycheck situation, where as long as our bills are paid every day, technically we think we’re normal. But we still feel this sense of health anxiety – if you will – like we just don’t know if my car breaks down, or my water heater breaks down, do I have enough money to pay these events in my life?
That’s what health feels like to a lot of people, because they’re just kind of getting by. From a health perspective, they’re considered normal, but they have no reserve capacity, and they have no vitality in terms of health.
Plasmalogens are a type of molecule that you build a savings account of, over years, over decades. Your heart builds them up, your brain builds them up, and you slowly accumulate them. Then when you get an oxidative stress like what’s happening now in today’s world with all the covid and myocarditis and brain fog – a lot of these things are being caused because that reserve of plasmalogens has been depleted.
We want plasmalogens for a longevity perspective. There are other situations that can have low plasmalogens, other things can really knock your plasmalogens down.
So you want to start early, you want to build a savings account, and you want to maintain it. Maintain health and function, and create a sustained surplus for optimal health, for optimal neuromuscular performance.”
A free educational series recorded in 2021-2022 available at https://drgoodenowe.com/dr-goodenowes-educational-seminars/ takes the viewer through underlying research and principles of Dr. Goodenowe’s approach to health. It’s advertised as lasting four hours, but took me two days to view.
The series’ discussions and references are background material to better understand later presentations and interviews. Points of interest included:
Seminar B100 shows that the metabolomic profile of people who regularly eat broccoli is different than others.
B109 clarifies how peroxisomal function is improved through resistance exercise and intermittent fasting.
C103 and C104 show how plasmalogens act against neurodegeneration (Parkinson’s disease and multiple sclerosis).
Texts below videos are additional information, not transcripts. C101 text is historically informative.
The B200 ProdromeScan tutorial will take more study. But unlike Labcorp tests, ordering a ProdromeScan requires using a practitioner in Dr. Goodenowe’s network.
I sent the following to Prodrome customer service earlier this month:
Please add me to your approved list for ProdromeScan.
Customer service replied:
“We only add health professionals to an approved list, not individuals.”
I responded:
Good morning. I looked at the websites of doctors who are associated with Dr. Goodenowe who are near me. All of them are too compromised for me to establish a doctor / patient relationship. But I’m glad they left up their blog posts from earlier this decade so I could see who they really were before I reached out to them.
I request an exception to the policy.
Customer service replied:
“There is no exception that can be made to this policy. You need to be a patient of a certified practitioner.”
I’ll escalate my request before my 90-day trial of Prodrome Glia and Neuro products ends so I can get an appropriate metabolomic status. Right now, I won’t involve someone I can’t trust just to know my ProdromeScan information that’s additional to next week’s Labcorp tests.
My treatment-result metabolomic data is probably not mature today on Day 29 of ProdromeGlia and ProdromeNeuro supplementation, resistance exercise, and intermittent fasting. I otherwise wouldn’t have experienced these two events:
I’m happy that after starting normal ProdromeGlia and ProdromeNeuro doses at Day 1, then taking a ProdromeGlia loading dose starting from Day 11, my sense of smell and taste improved by Days 13-14.
“We use NAC in the lab all the time because it stops an Nrf2 activation. So that weak pro-oxidant signal that activates Nrf2, you switch it off by giving a dose of NAC. It’s a potent antioxidant in that right, but it’s blocking signalling. And that’s what I don’t like about its broad use.”
If someone bombs themself everyday with antioxidants, they’re doing nothing to improve training of their endogenous systems’ defensive functions. What happens when they stop bombing? One example was a 2022 human study that found GlyNAC-induced improvements dissolved back to baseline after supplements stopped.
“TFEB activity is required for sulforaphane (SFN)-induced protection against both acute oxidant bursts and chronic oxidative stress. SFN-induced TFEB nuclear accumulation was completely blocked by pretreatment of cells by N-acetyl-cysteine (NAC), or by other commonly used antioxidants. NAC also blocked SFN-induced mRNA expression of TFEB target genes, as well as SFN-induced autophagosome formation.”
In this 2023 presentation for a professional audience, Dr. Dayan Goodenowe showed an example of what could be done (in the form of what he personally did at ages 53-54) to restore and augment brain structure and function over a 17-month period by taking plasmalogens and supporting supplements:
Follow the video along with its interactive transcript. Restorative / augmentative supplements included:
Forms of MRI used to document brain structure and function changes were:
Brain volume decreases are the rule for humans beginning at age 40. Dr. Goodenowe documented brain volume increases, which aren’t supposed to happen, but did per the below slide of overall results:
“From a global cortical volume and thickness perspective, 17 months of high-dose plasmalogens reversed ~15 years of predicted brain deterioration.”
Specific increased adaptations in brain measurements over 17 months included:
Cortical thickness .07/2.51 = +3%.
White matter microstructure fractional anisotropy +8%.
Neurovascular coupling signal controlled by noradrenaline integrity.
Amygdala volume +4% and its connectivity to the insula, indicating ongoing anxiety and emotional stress response.
Parahippocampus volume +7%.
Hippocampus fractional anisotropy +5%.
No changes:
Amygdala connectivity to the ventral lateral prefrontal cortex, the same part of the brain that relates to placebo effect.
Hippocampus connectivity.
Decreased adaptations in brain measurements included:
White matter microstructure radial diffusivity -10%.
Amygdala connectivity to the anterior cingulate cortex to suppress / ignore / deny anxiety response.
Amygdala connectivity to the dorsal lateral prefrontal cortex.
Entorhinal cortex volume -14%.
Hippocampus volume -6%.
Hippocampus mean diffusivity (white matter improved, with more and tighter myelin) -4%.
The other half of this video was a lively and wide-ranging Q&A session.
The referenced 2023 study of 653 adults followed over ten years showed what brain deterioration could be expected with no interventions. Consider these annual volume decrease rates to be a sample of a control group:
The daily plasmalogen precursor doses Dr. Goodenowe took were equivalent to 100 mg softgel/kg, double the maximum dose of 50 mg softgel/kg provided during the 2022 clinical trial of cognitively impaired old people referenced in Plasmalogens Parts 1, 2, and 3.
He mentions taking 5 ml in the morning and 5 ml at night because he used the Prodrome oil products. 1 ml of a Prodrome oil plasmalogen precursor product equals 900 mg of their softgel product.
“My brain is trying to minimize long-term effects of pain/stress by suppressing my memory of it. But this can only go on for so long before it becomes an entrenched state.
I have solved the sustenance side of the equation. I need to work harder to solve the environmental side.”
While I agree that we each have a responsibility to ourselves to create an environment that’s conducive to our health, the above phenomenon isn’t necessarily resolvable by changing an individual’s current environment. My understanding is that long-term effects of pain, stress, and related human experiences are usually symptoms of causes that started much earlier in our lives.
Adjusting one’s present environment may have immediate results, but probably won’t have much therapeutic impact on long-term issues. Early life memories and experiences are where we have to gradually go in order to stop being driven by what happened back then.
See Dr. Arthur Janov’s Primal Therapy for its principles and explanations. I started Primal Therapy at a similar age, 53, and continued for three years.
Two 2023 papers, starting with a study of smell and taste disorders:
“This study investigates the impact of etiology on the epidemiologic profile, disease severity, type of treatment, and therapy outcome in smell and taste disorders.
Hyposmia has a prevalence of about 15%, while approximately 5% of the population suffers from anosmia. Multiple innervation of the taste mucosa with fibers from the seventh, ninth, and tenth cranial nerves assures robustness of the gustatory system compared to smell.
Conservative therapy employs corticosteroids, antibiotics, vitamins and and minerals as well as functional rehabilitation by olfactory training. Data regarding outcome of therapy were only available for 71 (26.3%) of patients. Only the sinunasal etiology was significantly more likely to show improvement after therapy (27.4% show improvement vs. 9.6% show no improvement).”
This study was a little light on describing effective treatments for smell and taste problems. For example, olfactory training was said to have good therapeutic response. Looking it up, though, it seems to be whatever each practitioner feels like doing.
A review introduced the subject of olfactory ensheathing cells:
“Olfactory ensheathing cells (OECs) are glial cells of the primary olfactory nervous system, which are composed of the olfactory nerve and outer nerve fiber layer of the olfactory bulb. The primary olfactory nervous system is unique in that it can constantly regenerate.
It is now possible to remove olfactory bulb tissue and olfactory mucosa (outermost layer and lamina propria, which belong to the central nervous system and peripheral nervous system, respectively), which also suggests the potential value of OECs therapy in central nervous system and peripheral nervous system diseases. OECs can survive and renew in the central nervous system, and have been widely used in nerve regeneration and tissue repair.
Schwann cells (SCs) form the myelin sheath of the peripheral nerve, protect and nourish neurons, and play an irreplaceable role in the repair of peripheral nerve injury. There is no transcriptional difference between OECs and SCs. OECs are highly similar to SCs, and express the biomarkers of SCs.
Functional mechanisms of OECs in the treatment of neurological diseases include neuroprotection, immune regulation, axon regeneration, improvement of nerve injury microenvironment and myelin regeneration, which also includes secreted bioactive factors. Results obtained in clinical trials are not very satisfactory, and the effectiveness of these cell-based therapies remains to be proved.”
Something interesting may have unexpectedly started with my 90-day trial of Prodrome Glia and Neuro products. Here’s an abbreviated look that omits my intermittent fasting and resistance exercise data:
Both product labels have a loading dose suggestion of 4-8 softgels (2 to 4 times the standard two-softgel dose) for 1-3 months. Two days after I started a Glia loading dose, my sense of smell, then sense of taste, were noticeably better.
I’ll guess that my primary olfactory nervous system glial cells are responding to these changes. At the beginning I thought that my peripheral nervous system Schwann cells might be affected regarding my left ulnar nerve. Since olfactory ensheathing cells are highly similar to Schwann cells, it doesn’t seem to be that much of a stretch to think that they could also be affected by my current regimen.
More testing is warranted, of course. I’ve had diminished smell and taste for decades, though. If the gardenias, roses, magnolias, honeysuckles, and other scents in past summers that had fainter scents than I remembered come across stronger, so much the better.
The 2022 plasmalogen clinical trial mentioned in Parts 1 and 2 bypassed peroxisome metabolism of cognitively impaired people per discussion of the below diagram:
Increasing the body’s fasting state with time-restricted eating, and preventing muscle atrophy with resistance exercise, were offered as the two most important ways to improve peroxisomal function.
I didn’t find any relevant 2023 human studies (where I could access the full study) on different non-drug treatments that I was willing to do. A 2023 review outlined aspects of peroxisomes, to include a few older human studies:
“Peroxisomes are small, single-membrane-bound organelles, which are dynamic and ubiquitous. Peroxisomes directly interact with other organelles, such as endoplasmic reticulum, mitochondria, or lysosomes. Peroxisomes exert different functions in various cells through both catabolic and anabolic pathways.
The main functions of peroxisomes can be categorized as reactive oxygen species (ROS) metabolism, lipid metabolism, and ether-phospholipid biosynthesis. Peroxisomes also play important roles in inflammatory signaling and the innate immune response.”
1. Since I haven’t recently tried the two main ways to improve peroxisomal function, I’ll give them a go over the next three months:
Expect to get my feeding timeframe to within eight hours. Don’t know about making it short like 6 hours, because my first meal of the day is 35 calories of microwaved cruciferous sprouts, then I wait an hour before eating anything else.
Resistance exercise progress should be measurable, as I recorded exercises during the first ten weeks of eating broccoli sprouts every day 3.5+ years ago.
2. Don’t know that I’ll recognize any cognitive improvements to the extent I did during Week 9.
I don’t have a young brain anymore, and I’m sure some decline could be measured in memory tests. But I’m not going to become a lab rat.
There’s an occasional annoyance that’s been going on for some time, especially when I’m distracted. It happens when I think of something to do, and it somehow becomes a short-term memory that I did it, instead of going into a Things To Do queue. It’s largely self-correcting. For example, regardless of what I paid, I’ll drive back to the grocery store self-checkout to retrieve a third bag that didn’t make it home. A pink-haired employee said young people leave their paid-for groceries behind all the time. It’s usually more of a reality disconnect for me than forgetfulness, because I have a memory that I performed the action. Definitely room for improvement.
3. Don’t know that I’d see biochemical changes such as some described in Part 1. Maybe I’ll move up an annual physical to compare it with the last one in May?
I already have very little oxidative stress, very little inflammation, low triglycerides, high HDL, and no major improvements are indicated on CBC / CMP / lipid panels.
Take supplements to ensure other things like acetylcholine neurotransmitter availability, one-carbon / methylation metabolism, vitamin / mineral adequacy.
4. I started the two Prodrome plasmalogen precursor supplements (ProdromeGlia and ProdromeNeuro) a week ago, and take their standard doses. My thought is that resultant plasmalogens won’t degrade very much if their primary use isn’t to immediately address oxidative stress and inflammation. That could give these extra plasmalogens a chance to make larger homeostatic contributions in myelin and membrane areas.
I don’t expect any particular effects to manifest. But I’m interested to see if these two areas would be affected:
My left ulnar nerve has been giving me problems for over five years, and several resistance exercises aggravate it. I’ve had two nerve continuity tests during that time to confirm. Numbness and pain are intermittent, though.
I still take acetaminophen several times a day for other pain.
None of the above treatments are specifically indicated. But if time-restricted feeding and/or extra plasmalogens have an effect on left ulnar or other pain, maybe I’ll be able to make better progress on resistance exercise.