What does it take to empathetically understand, to make a part of oneself, to grok an ACE score?
The ACE effort was initiated in 1985 in an era before epigenetics was well-studied. Its artifacts included the ACE pyramid:
 The historical ACE lifespan continuum on the left began at conception. The pyramid on the right promoted a limited view of ACE that assigned childhood as the pyramid’s base.
The historical ACE lifespan continuum on the left began at conception. The pyramid on the right promoted a limited view of ACE that assigned childhood as the pyramid’s base.
Current official depictions of the ACE pyramid assign an expanded view of ACE as the pyramid’s base. The viewer’s attention is directed to “Scientific Gaps” between pyramid layers, but the largest gap remains: the continuum starts at conception but the pyramid still starts at childhood. The narrative claims:
“To provide scientific information that would be useful for developing new and more effective prevention programs.”
The official ACE pyramid doesn’t accurately reflect current science documented in, for example, Epigenetic effects of early life stress exposure. By downplaying Disrupted Neurodevelopment that may begin at conception, governing agencies implicitly endorse approaches that fail to address prenatal causes for later-life adverse effects.
If the ACE diagram was drawn thirty years later in 2015 to incorporate evidence for epigenetics, Disrupted Neurodevelopment wouldn’t be a consequent layer to an ACE base. The potential start of Disrupted Neurodevelopment would coincide with conception: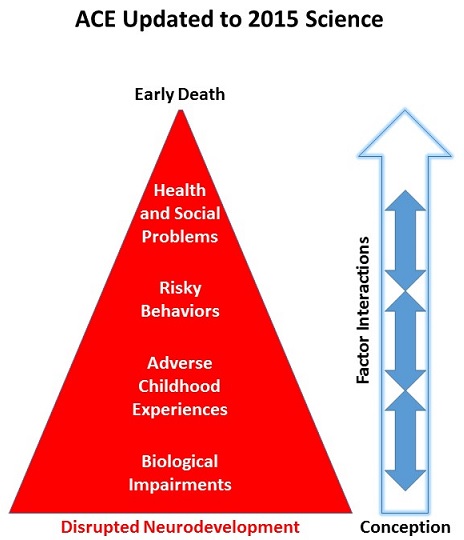
What’s an example of current ACE-related scientific evidence that wasn’t present three decades ago and also isn’t represented in the official ACE pyramid? Prenatal Disrupted Neurodevelopment may be considered today as a possible consequence of a “Yes” answer to half of the original ACE questions:
- Were your parents were too drunk or high to take care of you or take you to the doctor?
- Were your parents ever separated or divorced?
- Was your mother often or very often pushed, grabbed, slapped, or had something thrown at her?
- Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
- Was a household member depressed or mentally ill?
These threats and other stresses cause a fetus to biologically adapt. When such adaptations occur during prenatal development, they may:
- Have much larger impacts and
- Cause Biological Impairments that
- Don’t unassistedly disappear over time.
Emphasizing Disrupted Neurodevelopment that may begin at conception would encourage:
- Research that’s directed toward producing causal evidence for adaptations that largely occur during the early periods of an individual’s lifespan; and
- Research on how these adaptations consistently influence our later-life ideas, biology, and behavior.
The above recommendations for research are neither the current focus of ACE research nor the direction of related efforts to assist affected individuals. Relevant studies that I’ve curated on this blog often only produced symptomatic evidence:
- If a study couched its findings in non-etiologic phrases such as “is associated with” or “is linked to” or “may relate to,” it didn’t address ACE originating causes.
- “New and more effective prevention programs” seldom address Disrupted Neurodevelopment and Biological Impairments with efforts to reduce the source of the damage.
- If a program’s presentation showed multivariate analyses with ACE score probabilities and percentages, it didn’t address originating causes.
Here’s a YouTube search of ACE + adverse. Evaluate the current focus of ACE efforts by people employed in the social sciences and services. What did you notice?
How many presentations emphasized prenatal Disrupted Neurodevelopment, a period during which problems may be prevented by addressing causes? Did you instead see that these were outnumbered by many more presentations that emphasized Health and Social Problems symptom interventions?
So, what does it take to empathetically understand, to make a part of oneself, to grok a person’s ACE score?
Regarding empathy – it’s best to avoid the advice of studies such as:
- Problematic research: If you don’t feel empathy for a patient, is the solution to fake it? and
- If a study didn’t measure feelings, then its findings may not pertain to genuine empathy.
People who are helped may not recognize it at first, but over time, they’ll sense whether the helper’s empathy is genuine.
Regarding understanding – I feel that people first need to ameliorate the origins of their own problems. Then they may be able to help others therapeutically address causes for ACE symptoms.
Need proof? Think of someone you’ve met whose thoughts and feelings and behavior were caught up in and motivated by their own problems:
- Did you feel they could empathetically understand others?
- Wasn’t the welfare of the people who may have been helped truly incidental and secondary to someone who was acting out their own problems?