This 2015 Chicago review noted:
“Recent developments in the research of ASD [autistic spectrum disorder] with a focus on epigenetic pathways as a complement to current genetic screening.
Not all children with a predisposing genotype develop ASD. This suggests that additional environmental factors likely interact with the genome in producing ASD.
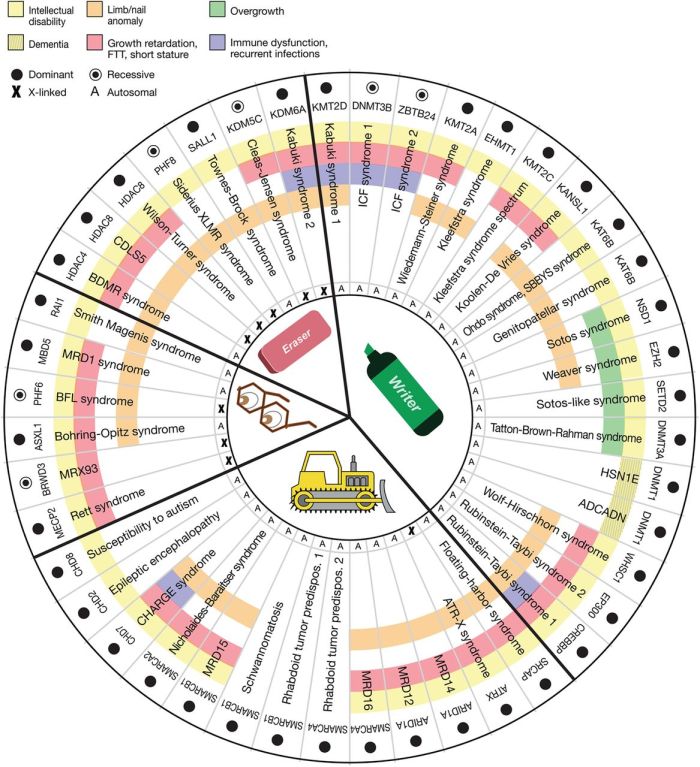
Increased risk of ASD is associated with mutations in genes that overlap with chromatin remodeling proteins, transcriptional regulators and synapse-associated proteins. Interestingly, these genes are also targets of environmentally induced changes in gene expression.”
Evidence was discussed for both broad and specific epigenetic ASD causes originating in the prenatal environment:
- Maternal stress:
“Prenatal stress exerts a profound epigenetic influence on GABAergic interneurons by altering the levels of proteins such as DNMT1 and Tet1 and decreasing the expression of various targets such as BDNF.
Ultimately, this results in reducing the numbers of fully functional GABAergic neurons postnatally and a concomitant increased susceptibility toward hyperexcitability. The delayed migration of GABAergic interneuron progenitors results in reduced gene expression postnatally which is likely the consequence of increased amounts of DNA methylation.
The net effect of stress during early development is to disrupt the balance of excitatory/inhibitory neuronal firing due to the loss of function associated with disrupted neuronal migration and maturation.”
- Prenatal nutrition:
“Exposure to a wide range of environmental toxins that impact neurodevelopment also result in global DNA hypomethylation. This model was extended to connect pathways between dietary nutrition and environmental exposures in the context of DNA hypomethylation. More recently, this hypothesis was expanded to show how dietary nutrients, environmental toxins, genome instability and neuroinflammation interact to produce changes to the DNA methylome.”
- Maternal infections:
“Inflammation, autoimmunity and maternal immune activation have long been suspected in the context of aberrant neurodevelopment and ASD risk.”
- Exposure to pollutants, medications, alcohol
This was a current review with many 2015 and 2014 references. However, one word in the reviewers’ vernacular that’s leftover from previous centuries was “idiopathic,” as in:
“Idiopathic (nonsyndromic) ASD, for which an underlying cause has not been identified, represent the majority of cases.”
It wasn’t sufficiently explanatory to use categorization terminology from thousands of years ago.
Science has progressed enough with measured evidence from the referenced studies that the reviewers could have discarded the “idiopathic” category and expressed probabilistic understanding of causes. They could have generalized conditional origins of a disease, and not reverted to “an underlying cause has not been identified.”
Another word the reviewers used was “pharmacotherapeutic,” as in:
“The goal for the foreseeable future is to provide a better understanding of how specific genes function to disrupt specific biological pathways and whether these pathways are amenable to pharmacotherapeutic interventions.”
Taking “idiopathic” and “pharmacotherapeutic” together – causes for the disease weren’t specifically identified, but the goal of research should be to find specific drug treatments?
Of course reviewers from the Department of Psychiatry, The Psychiatric Institute, University of Illinois at Chicago are biased to believe that “the design of better pharmacotherapeutic treatments” will fulfill peoples’ needs.
Are their beliefs supported by evidence? Without using drugs, are humans largely incapable of therapeutic actions such as:
- Preventing epigenetic diseases from beginning in the prenatal environment?
- Treating epigenetic causes for and alleviating symptoms of their own disease?
http://www.futuremedicine.com/doi/full/10.2217/epi.15.92 “Merging data from genetic and epigenetic approaches to better understand autistic spectrum disorder”