People will forgive you for being wrong, but they will never forgive you for being right – especially if events prove you right while proving them wrong. Thomas Sowell
“With memory encoding reliant on persistent changes in the properties of synapses, a key question is how can memories be maintained from days to months or a lifetime given molecular turnover? It is likely that positive feedback loops are necessary to persistently maintain the strength of synapses that participate in encoding.
These levels are not isolated, but linked by shared components of feedback loops.”
Despite the review’s exhaustive discussion, the reviewers never came to the point. The word cloud I made of the review’s most frequent thirty words had little to do with why memory occurs:
Why are almost all of the stimuli an organism receives not remembered?
Much of the discussion was baseless because it excluded emotion. Many of the citations’ memory findings relied on emotion, though.
For example, in the subsection Roles of persistent epigenetic modifications for maintaining LTF [long-term facilitation], LTP [long-term potentiation], and LTM [long-term memory]:
“Histone acetylation is increased after fear conditioning in the hippocampus and amygdala.
Correspondingly, inhibition of histone deacetylase enhances fear conditioning and LTP.
Following fear conditioning, histone phosphorylation is also increased.
DNA methylation is also up-regulated in the hippocampus and amygdala after fear conditioning, and inhibition of DNA methylation blocks fear LTM.”
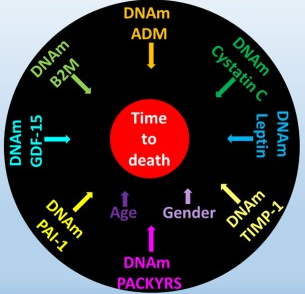
“DNAm GrimAge, a linear combination of chronological age, sex, and DNAm-based surrogate biomarkers for seven plasma proteins and smoking pack-years, outperforms all other DNAm-based biomarkers, on a variety of health-related metrics.
An age-adjusted version of DNAm GrimAge, which can be regarded as a new measure of epigenetic age acceleration (AgeAccelGrim), is associated with a host of age-related conditions, lifestyle factors, and clinical biomarkers. Using large scale validation data from three ethnic groups, we demonstrate that AgeAccelGrim stands out among pre-existing epigenetic clocks in terms of its predictive ability for time-to-death, time-to-coronary heart disease, time-to-cancer, its association with computed tomography data for fatty liver/excess fat, and early age at menopause.”
A miserable attempt at reporting the study’s findings included angles of superstition, fear-of-the-future, and suspicion-by-spurious-association:
“The research has already captured the attention of the life insurance industry. After all, a solid death date could mean real savings when it comes to pricing policies.
The hope is that if and when legitimate anti-aging drugs are developed, GrimAge could be used to test their effectiveness. In a world with functional anti-aging drugs, “doctors could test [your GrimAge number] and say, ‘You know what, you’re aging too quickly. Take this,'” Horvath said.”
A detailed blog post from Josh Mitteldorf provided scientific coverage of the study:
“Methylation sites associated with smoking history predicted how long the person would live more accurately than the smoking history itself. Even stranger, the methylation marks most closely associated with smoking were found to be a powerful indication of future health even when the sample was confined to non-smokers.
The DNAm GrimAge clock was developed in two stages, a correlation of a correlation. Curiously, the indirect computation yields the better result.
Horvath’s finding that secondary methylation indicators are more accurate than the underlying primary indicator from which they were derived is provocative, and calls out for a new understanding.”
When there are logical disconnects in findings like the above, it’s time to examine underlying premises. As noted in Group statistics don’t necessarily describe an individual, an assumption required by statistical analyses is that each measured item in the sample is interchangeable with the next.
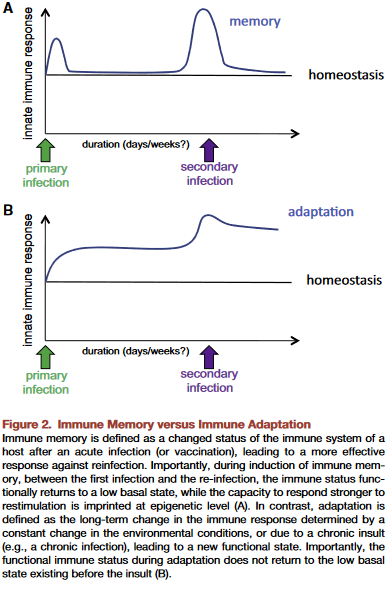
This presumption is often false, producing individually inapplicable results. For example, Immune memory vs. immune adaptation included this description of the adaptive immune system:
“To be effective, highly specific immune responserequires huge diversity of receptors and antibodies, which is achieved by somatic rearrangement of gene segments. Recombination results in millions of TCR [T cell receptor] and antibody variants able to recognize and neutralize millions of various antigens.”
Standard statistics of millions of T cell receptor and antibody variants won’t represent their individually unique properties. But individual differences are both their purpose and benefit to us.
The GrimAge study’s overreach was most apparent in stratifying educational attainment to develop correlations. As mentioned in Does a societal mandate cause DNA methylation? such statistics are poor evidence of each individual’s biological realities.
Neither derivatives of group statistics, nor correlations of correlations, seem to be the techniques needed to understand biological causes of effects. Another commentary on the GrimAge study mentioned but glossed over this point:
“It remains a mystery why exactly the epigenetic clocks work, and whether age-related changes in DNA methylation contribute to the cause of aging or are a result of it.”
This 2019 Dutch/German/Romanian perspective aimed for a better understanding of immune systems:
“Based on molecular, immunological, and evolutionary arguments, we propose that innate immune memory is a primitive form of immune memory present in all living organisms, while adaptive immune memory is an advanced form of immune memory representing an evolutionary innovation in vertebrates.
Innate immune responses have the capacity to be trained, and thereby exert a new type of immunological memory upon reinfection. The central feature of trained innate immune cells is their ability to mount a qualitatively and quantitatively different transcriptional response when challenged with microbes or danger signals. Evidence supports convergence of multiple regulatory layers for mediating innate immune memory, including changes in chromatin organization, DNA methylation, and probably non-coding RNAs such as microRNAs and/or long non-coding RNAs.
Two properties of adaptive immune response are mediated by two fundamentally different types of mechanisms:
Higher magnitude and speed of the response is mediated by epigenetic programming.
Specificity of the response is insured by gene recombination of TCR [T cell receptor] and BCR [B cell receptor] and clonal expansion of specific cell subpopulations upon antigen recognition.
To be effective, highly specific immune response requires huge diversity of receptors and antibodies, which is achieved by somatic rearrangement of gene segments. Recombination results in millions of TCR and antibody variants able to recognize and neutralize millions of various antigens.“
This paper included speculations such as “Evidence supports..probably non-coding RNAs” quoted above, and the penultimate sentence:
“One can envision that vaccines that are capable of inducing both forms of immune memory at the same time would be more effective.”
100% factual evidence is preferred. Overall information can only be as accurate as the least accurate information.
This 2019 McGill paper reviewed human and animal studies on brain-shaping influences from the fetal period through childhood:
“In neonates, regions of the methylome that are highly variable across individuals are explained by the genotype alone in 25 percent of cases. The best explanation for 75 percent of variably methylated regions is the interaction of genotype with different in utero environments.
A meta-analysis including 45,821 individuals with attention-deficit/hyperactivity disorder and 9,207,363 controls suggests that conditions such as preeclampsia, Apgar score lower than 7 at 5 minutes, breech/transverse presentations, and prolapsed/nuchal cord – all of which involve some sort of poor oxygenation during delivery – are significantly associated with attention-deficit/hyperactivity disorder. The dopaminergic system seems to be one of the brain systems most affected by perinatal hypoxia-ischemia.
Exposure to childhood trauma activates the stress response systems and dysregulates serotonin transmission that can adverselyimpact brain development. Smaller cerebral, cerebellar, prefrontal cortex, and corpus callosum volumes were reported in maltreated young people as well as reduced hippocampal activity.
Environmental enrichment has a series of beneficial effects associated with neuroplasticity mechanisms, increasing hippocampal volume, and enhancing dorsal dentate gyrus-specific differences in gene expression. Environmental enrichment after prenatal stress decreases depressive-like behaviors and fear, and improves cognitive deficits.”
The reviewers presented strong evidence until the Possible Factors for Reversibility section, which ended with the assertion:
“All these positive environmental experiences mentioned in this section could counterbalance the detrimental effects of early life adversities, making individuals resilient to brain alterations and development of later psychopathology.”
The review’s penultimate sentence recognized that research is seldom done on direct treatments of causes:
“The cross-sectional nature of most epigenetic studies and the tissue specificity of the epigenetic changes are still challenges.”
Cross-sectional studies won’t provide definitive data on cause-and-effect relationships.
The question yet to be examined is: How can humans best address these early-life causes to ameliorate their lifelong effects?
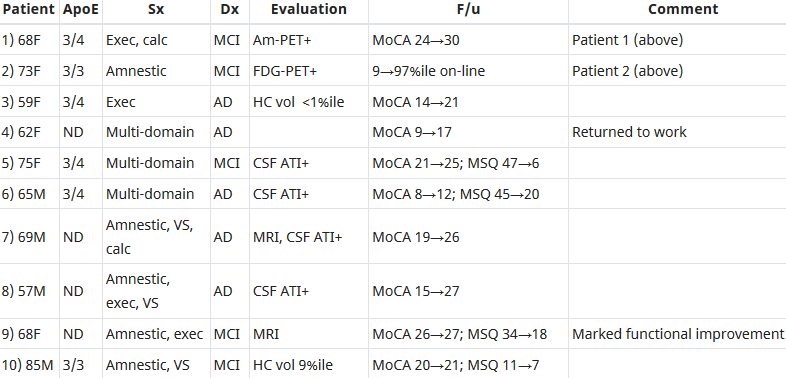
This 2018 human study presented the results of 100 patients’ personalized therapies for cognitive decline:
“The first examples of reversal of cognitive decline in Alzheimer’s disease and the pre-Alzheimer’s disease conditions MCI (Mild Cognitive Impairment) and SCI (Subjective Cognitive Impairment) have recently been published..showing sustained subjective and objective improvement in cognition, using a comprehensive, precision medicine approach that involves determining the potential contributors to the cognitive decline (e.g., activation of the innate immune system by pathogens or intestinal permeability, reduction in trophic or hormonal support, specific toxin exposure, or other contributors), using a computer-based algorithm to determine subtype and then addressing each contributor using a personalized, targeted, multi-factorial approach dubbed ReCODE for reversal of cognitive decline.
An obvious criticism of the initial studies is the small number of patients reported. Therefore, we report here 100 patients, treated by several different physicians, with documented improvement in cognition, in some cases with documentation of improvement in electrophysiology or imaging, as well.”
“We have a paper in press, due to appear 10.22.18 (open access, JADP, I’ll send a copy as soon as available), showing 100 patients with documented improvement – some with MRI volumetrics improved, others with quantitative EEG improvements, others with evoked response improvements, and all with quantitative cognitive assessment improvement. Some are very striking – 12 point improvements in MoCA [Montreal Cognitive Assessment], for example – others less so, but all also have subjective improvement. Hopefully this will address some of the criticisms that we haven’t documented improvement in enough people.
We were just turned down again for a randomized, controlled clinical trial, so on the one hand, we are told repeatedly that no one will believe that this approach works until we publish a randomized, controlled study, and on the other hand, we’ve been turned down (first in 2011/12, and now in 2018), with the complaint that we are trying to address more than one variable in the trial (as if AD is a single-variable disease!). Something of a catch-22. We are now resubmitting (unfortunately, the IRBs are not populated by functional medicine physicians, so they are used to seeing old-fashioned drug studies), and we’ll see what happens.
I’ve been extending the studies to other neurodegenerative diseases, and it has been impressive how much of a programmatic response there seems to be in these ‘diseases.’
I agree with you that there are many features in common with aging itself.
You made a good point that APP [amyloid precursor protein] is a dependence receptor, and in fact it functions as an integrating dependence receptor, responding to numerous inputs (Kurakin and Bredesen, 2015).
In the book and the publications, we don’t claim it is a “cure” since we don’t have pathological evidence that the disease process is gone. What we claim is ‘reversal of cognitive decline’ since that is what we document.
As I mentioned in the book, AD is turning out to be a protective response to multiple insults, and this fits well with the finding that Abeta has an antimicrobial effect (Moir and Tanzi’s work). It is a network-downsizing, protective response, which is quite effective – some people live with the ongoing degenerative process for decades.
We have seen several cases now in which a clinical trial of an anti-amyloid antibody made the person much worse in a time-dependent manner (each time there was an injection, the person would get much worse for 5-10 days, then begin to improve back toward where he/she was, but over time, marked decline occurred), and this makes sense for the idea that the amyloid is actually protecting against pathogens or toxins or some other insult.
It is important to note that we’ve never claimed that all people get better – this is not what we’ve seen. People very late in the process, or who don’t follow the protocol, or who don’t address the various insults, do not improve. It is also turning out to be practitioner dependent – some are getting the vast majority of people to improve, others very few, so this is more like surgery than old-fashioned prescriptive medicine – you have to do a somewhat complicated therapeutic algorithm and get it right for best results.
I’m very interested in what is needed to take the next step in people who have shown improvement but who started late in the course. For example, we have people now who have increased MoCA from 0 to 9 (or 0 to 3, etc.), with marked subjective improvement but plateauing at less than normal. These people had extensive synaptic and cellular loss prior to the program. So what do we need to raise the plateau? Stem cells? Intranasal trophic support? Something else?
I haven’t yet seen a mono-etiologic theory of AD or a mono-therapeutic approach that has repeatedly positive results, so although I understand that there are many theories and treatments, there doesn’t seem to be one etiology to the disease, nor does there seem to be one simple treatment that works for most. It is much more like a network failure.”
At a specific level:
“There doesn’t seem to be one etiology to the disease,
Nor does there seem to be one simple treatment that works for most.
We don’t have pathological evidence that the disease process is gone.”
For general concepts, however:
“AD is turning out to be a protective response to multiple insults.
It is a network-downsizing, protective response, which is quite effective.
The amyloid is actually protecting against pathogens or toxins or some other insult.”
For a framework of an AD cure to be valid, each source of each insult that evoked each “protective response” should be traced.
Longitudinal studies would be preferred inside this framework. These study designs would investigate evidence of each insult’s potential modifying effect on each “protective response” that could affect the cumulative disease trajectory of each individual.
In many cases, existing study designs would be adequate if they extended their periods to the end of the subjects’ natural lifetimes. One AD-relevant example would be extending the prenatally-restraint-stressed model used in:
The framework would also encourage extending studies to at least three generations to investigate evidence for transgenerational effects, as were found in:
This 2018 Chinese animal review subject was prenatal and perinatal anesthesia’s adverse epigenetic effects on a fetus/neonate:
“Accumulating evidence from rodent and primate studies has demonstrated that in utero or neonatal exposure to commonly used inhaled and intravenous general anesthetics is associated with neural degeneration and subsequent neurocognitive impairments, manifested in learning and memory disabilities.
So far, conflicting data exist about the effect of anesthetic agents on neurodevelopment in humans and no definite conclusion has been given yet.”
The inhibitors in the above graphic counter anesthesia’s effects on the fetus/neonate, summarized as:
“Epigenetic targeting of DNA methyltransferases and/or histone deacetylases may have some therapeutic value.”
Do physicians consider possible epigenetic alterations of a newborn’s chromatin structure and gene expression when they administer anesthesia to mothers during childbirth?
This 2016 US/Italy article was written from a perspective of regenerative bioengineering:
“Higher levels beyond molecular can have their own unique dynamics that offer better (e.g. more parsimonious and potent) explanatory power than models made at lower levels. Biological systems may be best amenable to models that include information structures (organ shape, size, topological arrangements and complex anatomical metrics) not defined at molecular or cellular level but nevertheless serving as the most causally potent ‘knobs’ regulating large-scale outcomes.
Top-down models can be as quantitative as familiar bottom-up systems biology examples, but they are formulated in terms of building blocks that cannot be defined at the level of gene expression and treat those elements as bona fide causal agents (which can be manipulated by interventions and optimization techniques). The near-impossibility of determining which low-level components must be tweaked in order to achieve a specific system-level outcome is a problem that plagues most complex systems.
The current paradigm in biology of exclusively tracking physical measurable and ignoring internal representation and information structures in patterning contexts quite resemble the ultimately unsuccessful behaviourist programme in psychology and neuroscience. For example, even if stem cell biologists knew how to make any desired cell type from an undifferentiated progenitor, the task of assembling them into a limb would be quite intractable.
Current state of the art in the field of developmental bioelectricity is that it is known, at the cellular level, how resting potentials are transduced into downstream gene cascades, as well as which transcriptional and epigenetic targets are sensitive to change in developmental bioelectrical signals. What is largely missing however is a quantitative understanding of how global dynamics of bioelectric circuits make decisions that orchestrate large numbers of individual cells, spread out over considerable anatomical distances, towards specific pattern outcomes.”
Regenerative research is gathering evidence for goal-directed memory and learning that doesn’t meet current definitions. For example:
“A tail grafted to the flank of a salamander slowly remodels to a limb, a structure more appropriate for its new location, illustrating shape homeostasis towards a normal amphibian body plan. Even tail tip cells (in red) slowly become fingers, showing that remodelling is not driven by only local information.”
These reviewers compared their findings to several existing research and real-world-operations domains. Other models may also benefit from concepts of:
“Quantitative, predictive, mechanistic understanding of goal-directed morphogenesis.”
I came across this article as a result of its citation in The Body Electric blog post.
“Levin drops a hint that there are photo-sensitive drugs that can control ion gates that can be used to translate a projected geometric image into a pattern of membrane potentials. He argues that the patterns encode ‘blueprints’ rather than a ‘construction manual’ based on the fact that the program is adaptive in the face of physical barriers and disruptions.”
“If sexually naïve females have their formative sexually rewarding experiences paired with the same male, they will recognize that male and display mate-guarding behavior towards him in the presence of a female competitor. Female rats that display mate-guarding behavior also show enhanced activation of oxytocin and vasopressin neurons in the supraoptic and paraventricular hypothalamic nucleus.
We examined the effect of a lysine-specific demethylase-1 inhibitor to block the action of demethylase enzymes and maintain the methylation state of corresponding genes. Female rats treated with the demethylase inhibitor failed to show any measure of mate guarding, whereas females treated with vehicle displayed mate guarding behavior. Demethylase inhibitor treatment also blocked the ability of familiar male cues to activate oxytocin and vasopressin neurons, whereas vehicle-treated females showed this enhanced activation.”
General principles and their study-specific illustrations were:
“Histone modifications are a key element in gene regulation through chromatin remodeling. Histone methylation / demethylation does not have straightforward transcriptional outcomes as do other histone modifications, like acetylation, which is almost invariably associated with transcriptional activation.
What is of vital importance in regards to histone methylation / demethylation is the pattern of methylation that is established. Patterns of methylation incorporate both methylated and demethylated residues, and are what ultimately play a role in transcriptional outcomes.
In the present study, inhibiting LSD1 demethylase enzymes disrupted the ability of cells to properly establish histone methylation / demethylation patterns, thus creating a deficit in the cells’ ability to transcribe the gene products necessary for the enhanced induction of OT, AVP, and the subsequent mate-guarding behaviors we observed. This study is the first to demonstrate a definitive role of epigenetic histone modifications in a conditioned sexual response.”
Wouldn’t it be nice if we were older Then we wouldn’t have to wait so long? And wouldn’t it be nice to live together In the kind of world where we belong?
You know it’s gonna make it that much better When we can say goodnight and stay together
Wouldn’t it be nice if we could wake up In the morning when the day is new? And after having spent the day together Hold each other close the whole night through?
Happy times together we’ve been spending I wish that every kiss was neverending Oh wouldn’t it be nice?
Maybe if we think and wish and hope and pray it might come true Baby then there wouldn’t be a single thing we couldn’t do We could be married (we could be married) And then we’d be happy (and then we’d be happy) Oh wouldn’t it be nice?
You know it seems the more we talk about it It only makes it worse to live without it But lets talk about it Oh wouldn’t it be nice?
A subset of memory recall–induced neurons in the DG [dentate gyrus] becomes reactivated after memory attenuation,
The degree of fear reduction positively correlates with this reactivation, and
The continued activity of memory recall–induced neurons is critical for remote fear memory attenuation.
Although other brain areas such as the prefrontal cortex and the amygdala are likely to be implicated in remote fear memories and remain to be investigated, these results suggest that fear attenuation at least partially occurs in memory recall–induced ensembles through updating or unlearning of the original memory trace of fear.
These data thereby provide the first evidence at an engram-specific level that fear attenuation may not be driven only by extinction learning, that is, by an inhibitory memory trace different from the original fear trace.
Rather, our findings indicate that during remote fear memory attenuation both mechanisms likely coexist, albeit with the importance of the continued activity of memory recall–induced neurons experimentally documented herein. Such activity may not only represent the capacity for a valence change in DG engram cells but also be a prerequisite for memory reconsolidation, namely, an opportunity for learning inside the original memory trace.
As such, this activity likely constitutes a physiological correlate sine qua non for effective exposure therapies against traumatic memories in humans: the engagement, rather than the suppression, of the original trauma.”
The researchers also provided examples of human trauma:
“We dedicate this work to O.K.’s father, Mohamed Salah El-Dien, and J.G.’s mother, Wilma, who both sadly passed away during its completion.”
So, how can this study help humans? The study had disclosed and undisclosed limitations:
1. Humans aren’t lab rats. We can ourselves individually change our responses to experiential causes of ongoing adverse effects. Standard methodologies can only apply external treatments.
2. It’s a bridge too far to go from neural activity in transgenic mice to expressing unfounded opinions on:
“A physiological correlate sine qua non for effective exposure therapies against traumatic memories in humans.”
Human exposure therapies have many drawbacks, in addition to being applied externally to the patient on someone else’s schedule. A few others were discussed in The role of DNMT3a in fear memories:
“Inability to generalize its efficacy over time,
Potential return of adverse memory in the new/novel contexts,
Context-dependent nature of extinction which is widely viewed as the biological basis of exposure therapy.”
3. Rodent neural activity also doesn’t elevate recall to become an important goal of effective human therapies. Clearly, what the rodents experienced should have been translated into human reliving/re-experiencing, not recall! Terminology used in animal studies preferentially has the same meaning with humans, since the purpose of animal studies is to help humans.
4. The researchers acknowledged that:
“Other brain areas such as the prefrontal cortex and the amygdala are likely to be implicated in remote fear memories and remain to be investigated.”
“The findings imply that in response to traumatic stress, some individuals, instead of activating the glutamate system to store memories, activate the extra-synaptic GABA system and form inaccessible traumatic memories.”
The study I curated yesterday, Organ epigenetic memory, demonstrated organ memory storage. It’s hard to completely rule out that other body areas may also store traumatic memories.
The wide range of epigenetic memory storage vehicles is one reason why effective human therapies need to address the whole person, the whole body, and each individual’s entire history.
This post has somehow become a target for spammers, and I’ve disabled comments. Readers can comment on other posts and indicate that they want their comment to apply here, and I’ll re-enable comments.
This 2018 Japanese review subject was the relationships of organ memory and non-communicable diseases:
“Organ memory is the engraved phenotype of altered organ responsiveness acquired by a time-dependent accumulation of organ stress responses. This phenomenon is known as “metabolic memory” or “legacy effect,” which is similar to neuronal and immune memory.
Not only is the epigenetic change of key genes involved in the formation of organ memory but the alteration of multiple factors, including low molecular weight energy metabolites, immune mediators, and tissue structures, is involved as well. These factors intercommunicate during every stress response and carry out incessant remodeling in a certain direction in a spiral fashion through positive feedback mechanisms.
The systematic review revealed that each intervention type, that is:
Glucose lowering,
Blood pressure lowering, or
LDL-cholesterol lowering,
possessed unique characteristics of the memory phenomenon. Most of the observational periods of these studies lasted for > 10 years. Memory phenomenon was suggested to last for a long time and is thought to have a considerable effect on the clinical course of NCDs [non-communicable diseases].
Organs cannot possess consciousness, so it might not be appropriate to consider whether a recalling process exists in organs. However, the properties of organs are incessantly altered by external stimuli loaded on organs as if it is updating.
It is clinically important to investigate whether organ memory can be updated by our behaviors. Once organ memory is established in an organ, organ memory in each organ can influence one another and affect organ memory in a different organ.
Epigenome-modification enzymes, such as histone deacetylases and DNA methyltransferases, and transcription factors seem to be essential for the epigenetic regulation of gene expression, which is involved in the generation of organ memory. Cellular metabolism can epigenetically modulate the expression of genes that are related to the progression of diseases.”
“Organs cannot possess consciousness, so it might not be appropriate to consider whether a recalling process exists in organs.”
Memory studies don’t require this consciousness to investigate even brain areas and functions. Researchers observe memory by measuring stimulus/response items like neuron activation and various levels of behavior. Consciousness is an emergent property.
2. Regarding recall: An organ’s “engraved phenotype of altered organ responsiveness” may not have recall itself, but it doesn’t have a separate existence apart from its body. An organ can’t be removed from its body for very long and still be part of its body.
When an organ is in its normal state as part of a body, it has access to recall-like functions via “inter-organ communication of organ memory.” The review also mentioned:
“Organ memory in each organ can influence one another and affect organ memory in a different organ.
Evolution didn’t support unnecessary duplication for a kidney’s memory to include recall because it’s part of a body that includes a brain that has recall. Evolution didn’t duplicate functions of a kidney’s memory in a brain, either.
It’s dawned on me that although links in blog posts are indexed by search engines, links in comments may not be. Here’s a post to elevate links in three comments that may have escaped notice.
“It is my view that all researchers have a narrow focus on what they want to research, without having an over-riding paradigm in which to fit the research and its results. Janovian Primal Therapy and theory, with its focus and understanding of the three different levels of consciousness would provide for a much needed over-arching paradigm, especially in the area of mental health.”
“You are right on. The Norcross survey, in particular, is utter crap. More than half of those “experts” surveyed were CBT therapists who knew nothing about PT and yet deemed themselves confident to judge “primal scream therapy” as “discredited.” I feel the therapy will never be understood for what it is.”
“There is of course, reversibility. Michael Meaney’s baby rats had their epigenetic changes reversed with loving maternal care. There are several compounds in development which have been shown to reverse methylation. This former physician and researcher says, “Epigenetic changes affect the level of activity of our genes. Genetic activity levels affect our emotions, beliefs, and our bodies. Exploring epigenetics and chronic illness may help us understand causes that many of us suspect have played a role in the onset and evolution of our illnesses. Furthermore, these epigenetic changes have been found to be reversible, at least some of the time, even with a seemingly indirect treatment such as psychotherapy.” Epigenetics and Chronic Illness: Why Symptoms May Be Reversible
So what gives? I suspect that your researcher is working with his/her head in the sand, hamstrung by their ideological biases. If CBT can effect epigenetic changes, imagine what primal therapy can do.”
And a seven-year anniversary repost of events that affect me every day:
This 2017 UC Irvine human review subject provided details of how fetalhypothalamic-pituitary-adrenal components and systems develop, and how they are epigenetically changed by the mother’s environment:
“The developmental origins of disease or fetal programming model predicts that intrauterine exposures have life-long consequences for physical and psychological health. Prenatal programming of the fetal hypothalamic-pituitary-adrenal (HPA) axis is proposed as a primary mechanism by which early experiences are linked to later disease risk.
Development of the fetal HPA axis is determined by an intricately timed cascade of endocrine events during gestation and is regulated by an integrated maternal-placental-fetal steroidogenic unit. Mechanisms by which stress-induced elevations in hormones of maternal, fetal, or placental origin influence the structure and function of the emerging fetal HPA axis are discussed.
Human gestational physiology and fetal HPA axis development differ even from that of closely related nonhuman primates, thereby limiting the generalizability of animal models. This review will focus solely on studies of prenatal stress and fetal HPA axis development in humans.”
1. Every time I read a prenatal study I’m in awe of all that has to go right – and at the appropriate times and sequences – for a fetus to be undamaged. Add in what needs to happen at birth, during infancy, and throughout early childhood, and it seems impossible for any human to escape epigenetic damage.
2. The reviewers referenced animal studies and human research performed with postnatal subjects, despite the disclaimer:
This review will focus solely on studies of prenatal stress and fetal HPA axis development in humans.”
This led to blurring of what had been studied or not with human fetuses regarding the subject.
3. These reviewers uncritically listed many dubious human studies that had both stated and undisclosed severe limitations on their findings. Other reviewers offer informed analysis of cited studies, as Sex-specific impacts of childhood trauma summarized with cortisol:
“Findings are dependent upon variance in extenuating factors, including but not limited to, different measurements of:
presence and severity of psychopathology symptomology.”
4. The paper would have been better had it stayed on topic with its title “Developmental origins of the human hypothalamic-pituitary-adrenal axis.” Let other reviews cover animals, post-natal humans, and questionable evidence.
5. I asked the reviewers to provide a searchable file to facilitate using their work as a reference.
This 2018 US government rodent study used extreme dosages to achieve its directed goals of demonizing nicotine and extolling the biomarker paradigm:
“This study examined whether adolescent nicotine exposure alters adult hippocampus-dependent learning, involving persistent changes in hippocampal DNA methylation and if choline, a dietary methyl donor, would reverse and mitigate these alterations.
Mice were chronically treated with nicotine (12.6mg/kg/day) starting at post-natal day 23 (pre-adolescent), p38 (late adolescent), or p54 (adult) for 12 days followed by a 30-day period during which they consumed either standard chow or chow supplemented with choline (9g/kg).
Our gene expression analyses support this model and point to two particular genes involved in chromatin remodeling, Smarca2 and Bahcc1. Both Smarca2 and Bahcc1 showed a similar inverse correlation pattern between promoter methylation and gene expression.
Our findings support a role for epigenetic modification of hippocampal chromatin remodeling genes in long-term learning deficits induced by adolescent nicotine and their amelioration by dietary choline supplementation.”
Let’s use the average weight of a US adult male – published by the US Centers for Disease Control as 88.8 kg – to compare the study’s dosages with human equivalents:
Nicotine at ((“12.6mg/kg/day” x .081) x 88.8 kg) = 90.6 mg.
Neither of these dosages are even remotely connected to human realities:
The human-equivalent dosage of nicotine used in this study would probably kill an adult human before the end of 12 days.
What effects would an adult human suffer from exceeding the choline “Tolerable Upper Intake Level” BY 18 TIMES for 30 days?
Isn’t the main purpose of animal studies to help humans? What’s the justification for performing animal studies simply to promote an agenda?
A funding source of this study was National Institute on Drug Abuse (NIDA) Identification of Biomarkers for Nicotine Addiction award (T-DA-1002 MG). Has the biomarker paradigm been institutionalized to the point where research proposals that don’t have biomarkers as goals aren’t funded?