A 2025 rodent study investigated sulforaphane’s effects on diabetic cardiomyopathy:
“The protective effect of cruciferae-derived sulforaphane (SFN) on diabetic cardiomyopathy (DCM) has garnered increasing attention. However, no studies have specifically explored its mechanistic involvement in cardiac substrate metabolism and mitochondrial function.
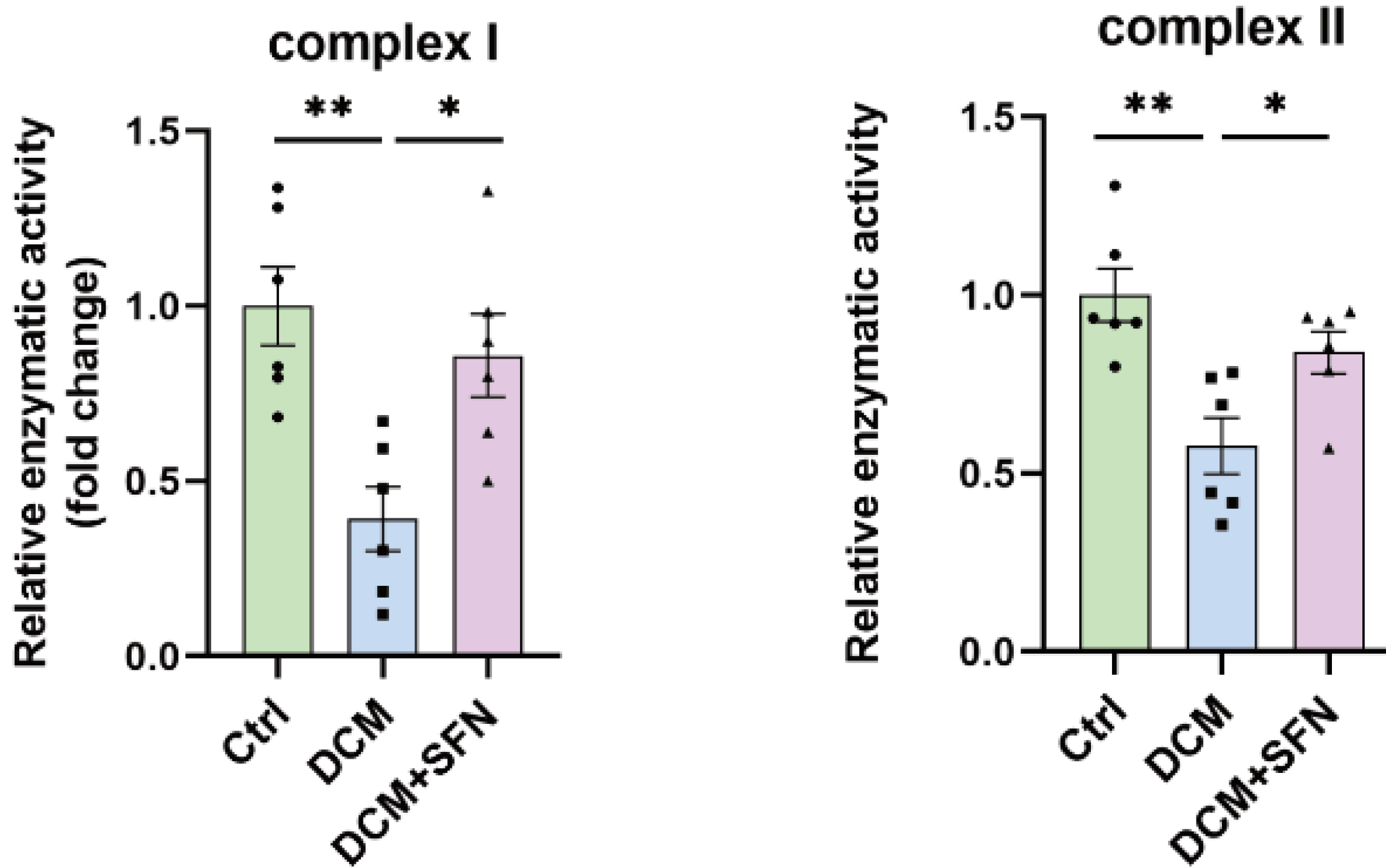
To address this gap, Type 2 diabetes mellitus (T2DM) db/db mice were orally gavaged with vehicle or 10 mg/kg body weight SFN every other day for 16 weeks, with vehicle-treated wild-type mice as controls. SFN intervention (SFN-I) alleviated hyperglycemia, dyslipidemia, HOMA-IR, serum MDA levels, and liver inflammation. SFN-I improved the lipotoxicity-related phenotype of T2DM cardiomyopathy, manifested as attenuation of diastolic dysfunction, cardiac injury, fibrosis, lipid accumulation and peroxidation, ROS generation, and decreased mitochondrial complex I and II activities and ATP content.
Although not fully understood, multiple systemic and cardiac-local mechanisms contribute to DCM, encompassing hyperglycemia, dyslipidemia, insulin resistance (IR), disturbances in cardiac substrate metabolism, lipotoxicity, glucotoxicity, mitochondrial dysfunction, oxidative stress, inflammation, and endoplasmic reticulum (ER) stress. Nrf2 and its downstream metallothionein also mediated the preventive effect of SFN on DCM, and may underlie the synergistic effect of SFN and zinc in DCM.
These results suggest that chronic oral SFN-I protects against DCM by mitigating overall metabolic dysregulation and inhibiting cardiolipotoxicity. The latter might involve controlling cardiac fatty acid metabolism and improving mitochondrial function, rather than promoting glucose metabolism.”
https://www.mdpi.com/2076-3921/14/5/603 “Oral Sulforaphane Intervention Protects Against Diabetic Cardiomyopathy in db/db Mice: Focus on Cardiac Lipotoxicity and Substrate Metabolism”
This study had numerous charts like the above showing it was better to not have a deviation from health (Ctrl) rather than incur injury (DCM) then try to fix it with sulforaphane (DCM + SFN). But the control group was wild-type mice, not mice genetically inclined to diabetes like the treatment groups.
The subjects’ starting points were at nine-weeks-old (equivalent to 18-25 year-old humans), and duration was 16 weeks. Grok 3 said: “A 25-week-old db/db mouse is roughly equivalent to a human aged 30–35 years chronologically, though its metabolic condition may mimic older human physiological states in diabetes and obesity research.”
A human equivalent of a 10 mg/kg sulforaphane dose is (.081 x 10 mg) = 56 mg orally administered every other day. That’s about how much total sulforaphane I estimated I took every day (52 mg) from Week 6 through Week 56 by eating microwaved broccoli sprouts twice daily.
No rationale was provided for the sulforaphane dose or the every-other-day dosing regimen. Since I took ~52 mg every day for almost a year, I’ll guess that this study may have had more definitive results with daily dosing. Or maybe add zinc per Zinc and broccoli sprouts – a winning combination.