A 2025 human study followed up Eat broccoli sprouts for your high intensity interval training using red kale sprouts:
“Glucosinolate-rich broccoli sprouts combined with intense exercise training for 7 days have been shown to reduce blood lactate concentrations during exercise, attenuate hypoglycemic events, improve physical performance, and reduce markers of oxidative stress. This study aimed to investigate the acute, dose-dependent effects of glucosinolate-rich red kale sprouts (GRS) on blood lactate and blood glucose following the ingestion of three different doses.
Fifteen healthy participants [11 females, 4 males] consumed 37.5 g or 75 g of GRS or an isocaloric placebo blended into a beverage on three separate occasions. The participants cycled on an ergometer at three submaximal work rates before and three hours after ingestion.
Intake of glucosinolate-rich sprouts acutely decreased blood lactate levels during submaximal cycling and increased blood glucose levels at rest. The largest reduction in blood lactate was observed at the 37.5 g dose compared to placebo.
To identify the dose of GRS that results in the lowest blood lactate concentration during submaximal exercise, we applied a quadratic modeling approach. The optimal dose for minimizing lactate accumulation was calculated as 44 g of GRS.

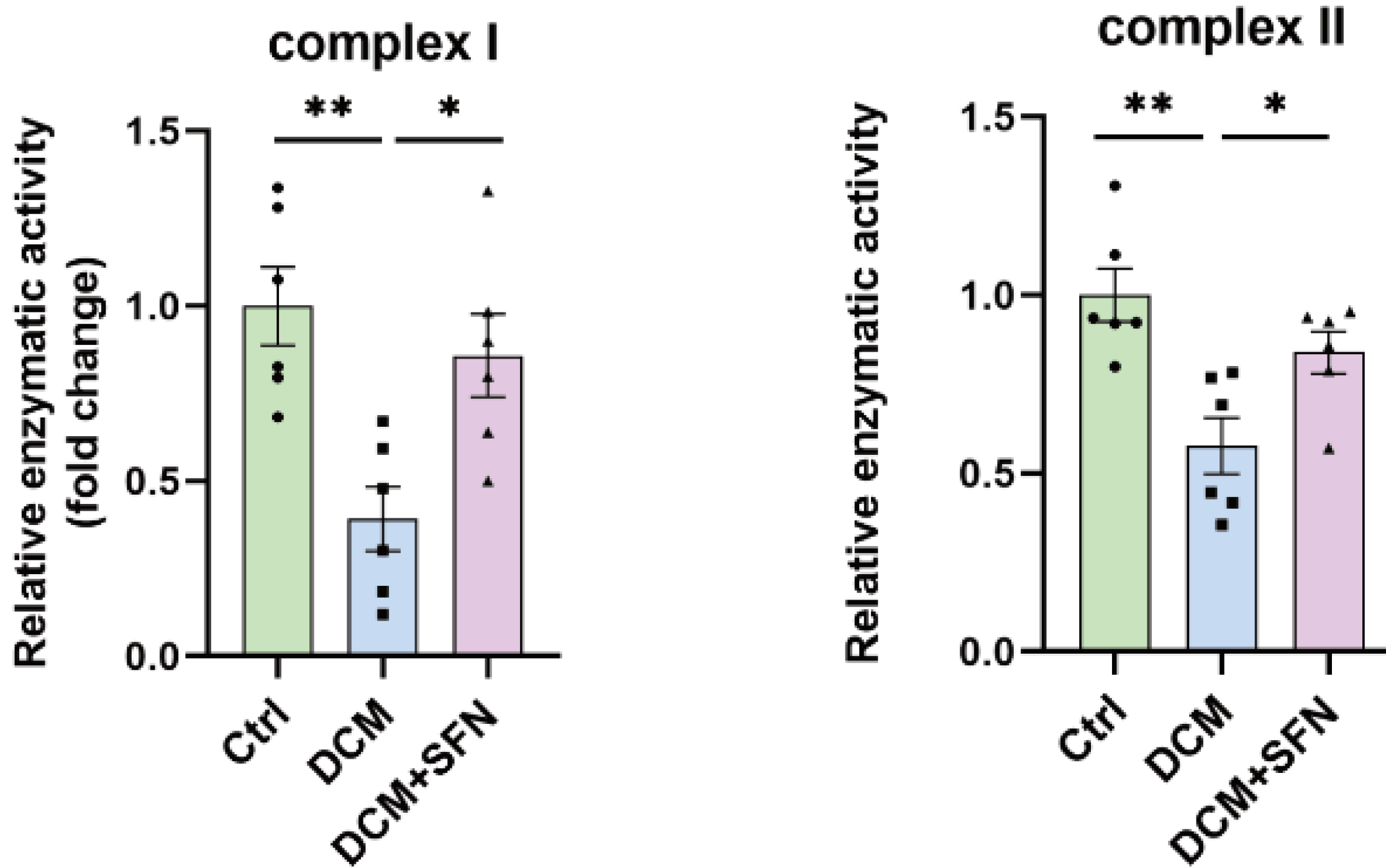
In our previous study, we found a tendency towards a lower respiratory exchange ratio after one week of supplementation. Moreover, studies have demonstrated that mitochondrial oxidation of long-chain and short-chain fatty acids is depressed in the absence of Nrf2, and accelerated when Nrf2 is constitutively active.
We observed a reduction in myeloperoxidase levels approximately three hours after GRS intake, suggesting a decrease in oxidative stress. This finding indicates that the adaptive compensatory system may act rapidly, likely within just a few hours of GRS consumption.
A limitation is that we did not assess whether the lower lactate levels translated into improved performance. Theoretically, if the reduction in lactate results from the activation of pyruvate dehydrogenase, it could enhance performance by channeling more pyruvate into mitochondria for efficient oxidation, reducing reliance on glycolysis, and thereby sparing muscle glycogen. Alternatively, if the lower lactate levels are due to increased activity of the hepatic Cori cycle, lactate could be more rapidly converted to glucose, possibly supporting glycogen resynthesis or maintaining blood glucose levels during exercise. Both mechanisms could potentially contribute to improved performance.
Acute intake of small doses of GRS followed by submaximal ergometer cycling results in changes in lactate and glucose metabolism that could be beneficial for exercise performance.”
https://www.biorxiv.org/content/10.1101/2025.04.15.648889v1.full “A glucosinolate-rich beverage lowers blood lactate concentrations during submaximal exercise”
These researchers chose red kale sprouts of undisclosed age over the predecessor study’s broccoli raab five-day old sprouts, and two other undisclosed cruciferous vegetable sprouts.
This study is in its preprint phase. Items that could be clarified before publishing in final form include:
- In the Abstract section, reference findings to red kale sprouts rather than broccoli sprouts;
- Characterize the lactate U-shaped dose-response curve as hormesis; and
- Reference other hormesis findings for context.