Two papers on Vitamin K2, and an online database to continue Part 1:
“Precise quantitative assessments of vitamin K bioavailability in humans is challenging due to unquantified tissue conversion of PK [phylloquinone, Vitamin K1] to MK [menaquinone, Vitamin K2]-4, and contributions of gut microbiota. Absorption of long-chain MKs (MK-7, MK-8 and MK-9) from natto, cheese and egg yolk is close to 100%.
Long-chain MKs have a longer half-life. Long half-life may not necessarily indicate increased bioavailability, but instead non-preferential utilisation by tissues compared to PK and MK-4. A long half-life may also indicate that long-chain MKs may be of particular importance for extrahepatic tissues.
12 databases list vitamin K content of individual food items, which is required to more accurately determine vitamin K intake. The Dutch database is the most comprehensive, and includes PK and several types of MKs, ranging from MK-4 to MK-10.”
https://pubs.rsc.org/en/content/articlelanding/2020/FO/C9FO02321F “Quantifying dietary vitamin K and its link to cardiovascular health: a narrative review” (not freely available)
One online database mentioned is at https://www.rivm.nl/en/dutch-food-composition-database:
“The Dutch Food Composition Database (NEVO) contains data on the composition of foods eaten frequently by a large part of the Dutch population. These foods contribute significantly to the intake of energy and nutrients. Foods of importance for specific groups of the Dutch population are also included.
The NEVO online website contains data on 133 nutrients of 2152 food items. The most recent version of NEVO online dates from November 2019.”
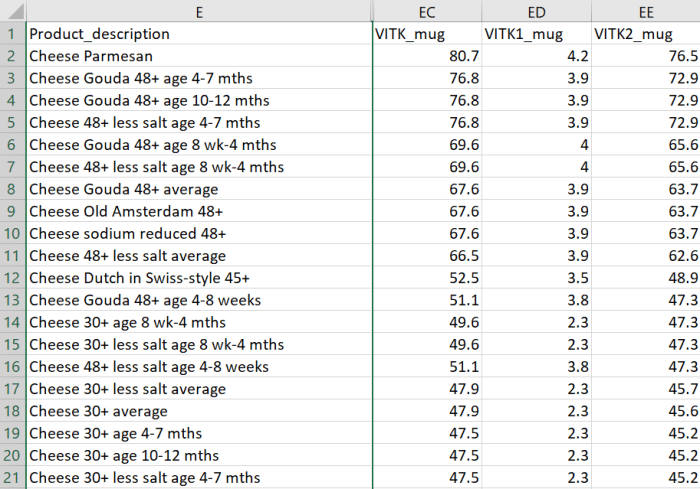
I downloaded a copy in Excel format, selected all, and sorted by column EE “VITK2_mug” in descending order. There were 263 food items with Vitamin K2 measurements.
A second paper detailed a 2021 double-blind, placebo-controlled, feasibility study:
“INTRICATE will assess the influence of combined vitamin K2 and vitamin D3 supplementation on micro-calcification in carotid artery disease. Considering recent advancements in medical imaging, ultrasound, PET/MRI, and computed tomography can be used for selection and stratification of patients with atherosclerosis.
Subjects will be randomized (1:1) to a vitamin K2 (400 µg MK-7/day) and vitamin D3 (80 µg [3200 IU]/day) dose or to placebo. Primary endpoint is change in Na[18F]F PET/MRI (baseline vs. after 3 months) in treatment group as compared to placebo arm. Secondary endpoints are changes in plaque composition and in blood-biomarkers.
Studies suggest positive effects of vitamin D on vitamin K-dependent metabolism. The MGP-gene promoter contains a vitamin D response element, capable of a two to threefold enhanced MGP expression after vitamin D binding.
Upregulation of MGP due to vitamin D needs vitamin K to ensure full activation of MGP for optimal functioning. This implies that the combination of both vitamin K and vitamin D could provide enhanced protection against progressive vascular calcification, cardiovascular disease, and mortality.”
https://www.mdpi.com/2072-6643/13/3/994/htm “Effects of Combined Vitamin K2 and Vitamin D3 Supplementation on Na[18F]F PET/MRI in Patients with Carotid Artery Disease: The INTRICATE Rationale and Trial Design”
The second study was somewhat of a tell in that after two decades, researchers are still testing Vitamin K2 dose efficacy. Researchers don’t consider it proper science to not use a statistics package to lump subjects into groups.
Someday researchers will thoroughly analyze each individual, and relate measurements to each individual’s causal and symptomatic characteristics. Then we’ll find out whether what did or didn’t matter to each individual, will or won’t matter to a group.
Until then they’ll focus on one dimension of health like Vitamin K2 foods per their sponsor’s directions. Nevermind that Vitamin K2-rich foods like cheeses are full of advanced glycation end products (AGEs) that humans can’t adequately metabolize, to our detriment.
