A trio of papers, with the second and third citing a 2013 review:
“The relationship between pain and hypertension is potentially of great pathophysiological and clinical interest, but is poorly understood. Perception of acute pain initially plays an adaptive role, which results in prevention of tissue damage.
The consequence of ascending nociception is recruitment of segmental spinal reflexes through physiological neuronal connections:
- In proportion to magnitude and duration of the stimulus, these spinal reflexes cause sympathetic nervous system activation, which increases peripheral resistances, heart rate, and stroke volume; and
- The response also involves the neuroendocrine system, in particular, the hypothalamic-pituitary-adrenal axis, in addition to further activation of the sympathetic system by adrenal glands.
Persistent pain tends to become chronic and to increase BP values. After a long time, dysfunction of release of endogenous opioids results in a reduction of their analgesic effect. A vicious circle is established, where further pain leads to a reduction in pain tolerance, associated with decreased analgesia mediated by baroreceptors, in a kind of process of exhaustion.”
https://onlinelibrary.wiley.com/doi/epdf/10.1111/jch.12145 “The Relationship Between Blood Pressure and Pain”
A second paper was a 2021 human experimental pain study:
“We investigated the effectiveness of physiological signals for automatic pain intensity estimation that can either substitute for, or complement patients’ self-reported information. Results indicate that for both subject-independent and subject-dependent scenarios, electrodermal activity (EDA) – which is also referred to as skin conductance (SC) or galvanic skin response – was the best signal for pain intensity estimation.
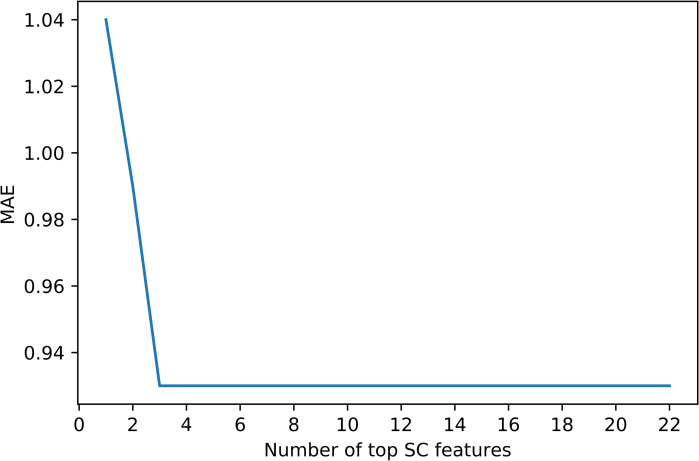
EDA gave mean absolute error (MAE) = 0.93 using only 3 time-series features:
- Time intervals between successive extreme events above the mean;
- Time intervals between successive extreme events below the mean; and
- Exponential fit to successive distances in 2-dimensional embedding space.
Although we obtained good results using 22 EDA features, we further explored to see if we could reach similar or better results with fewer EDA features. This plot highlights that by considering only the top 3 features, we obtained the same level of performance given by all 22 features together.
This is the first study that achieved less than 1-unit error for continuous pain intensity estimation using only one physiological sensor’s 3 time-series feature, and a Support Vector Regression machine learning model. Considering that this is an encouraging result, we can estimate objective pain using only the EDA sensor, which needs neither a complex setup nor a complex computationally intense machine learning algorithm.
This study paves the way for developing a smart pain measurement wearable device that can change the quality of pain management significantly.”
https://doi.org/10.1371/journal.pone.0254108 “Exploration of physiological sensors, features, and machine learning models for pain intensity estimation”
A third paper was a 2020 human rotator cuff surgery study:
“Results of our study demonstrated that:
- Pain during the early postoperative period;
- Time until occurrence of a retear; and
- Existence of hypertension
were correlated with severity of pain in patients with a retorn rotator cuff.
Pain was selected as the sole outcome parameter of this study because:
- Pain is an important factor that compels patients to seek treatment for rotator cuff tears, along with functional disability;
- Pain and subjective functional deficits are important factors that influence a surgeon’s decision to continue with treatment in cases of retearing; and
- Analyzing pain severity can be a good way to determine patients’ overall satisfaction after rotator cuff repair.
However, pain is not always correlated with disease severity or tear size and vice versa. A lack of pain does not necessarily depend on integrity of the repaired tendon or constitute a good prognosis. In fact, patients with partial-thickness rotator cuff tears showed more pain than did those with full-thickness tears.
Existence of hypertension had a proportional relationship with pain at 12 months postoperatively in patients with retears. This can be interpreted as a suggestion that pain in patients with retears is not acute, but rather chronic, and may be connected to pain in the early postoperative period at 3 months. However, results of this study cannot explain benefits of controlling hypertension in alleviating pain in patients with retears.”
https://journals.sagepub.com/doi/10.1177/2325967120947414 “Factors Related to Pain in Patients With Retorn Rotator Cuffs: Early Postoperative Pain Predicts Pain at 12 Months Postoperatively”

